A Patient I’ll Call James
James walked into my office in Petaluma fourteen months after a rear-end collision on Old Redwood Highway. He didn’t think he had a problem with his neck anymore. The acute pain had faded a year ago. He’d stopped taking ibuprofen. He’d stopped seeing his original chiropractor. By every measure he could think of, he’d recovered.
His wife had insisted he come in.
She’d been telling him for months that he’d “gotten weird about turning his head.” When he backed the car out of the driveway, he turned his whole body in the seat instead of glancing over his shoulder. When she said his name from the kitchen while he was at the stove, he’d swivel his torso to answer her. When he played with their kids on the rug, he’d lean down with a strangely flat back, like a man bending over a counter. He didn’t notice any of it. It felt totally normal to him.
What he did notice — when she pushed him to think about it — was that his shoulders had been aching, his low back had been tight after long drives, his right hip had started hurting when he ran, and he’d had a string of headaches he’d been blaming on screen time. None of it, in his mind, had anything to do with the crash. The crash was old news.
Here’s what I had to tell James, and what I want to tell you if you’ve been in a collision in the last year or two: your body adapts to injury whether you give it permission to or not. It rewrites the way you move, the way you hold yourself, the way you turn your head, and it does this entirely below the level of conscious awareness. The acute pain is the alarm. The compensation that follows is the permanent change. And the compensation, untreated, is what becomes the chronic syndrome that shows up two years later as a “different” problem in a “different” part of the body.
Awareness — bringing those silent compensations back to the surface where you can see them and change them — is one of the most underrated forms of medicine in the entire post-trauma toolkit. Let me explain why.
What “Adapting Without Awareness” Actually Means
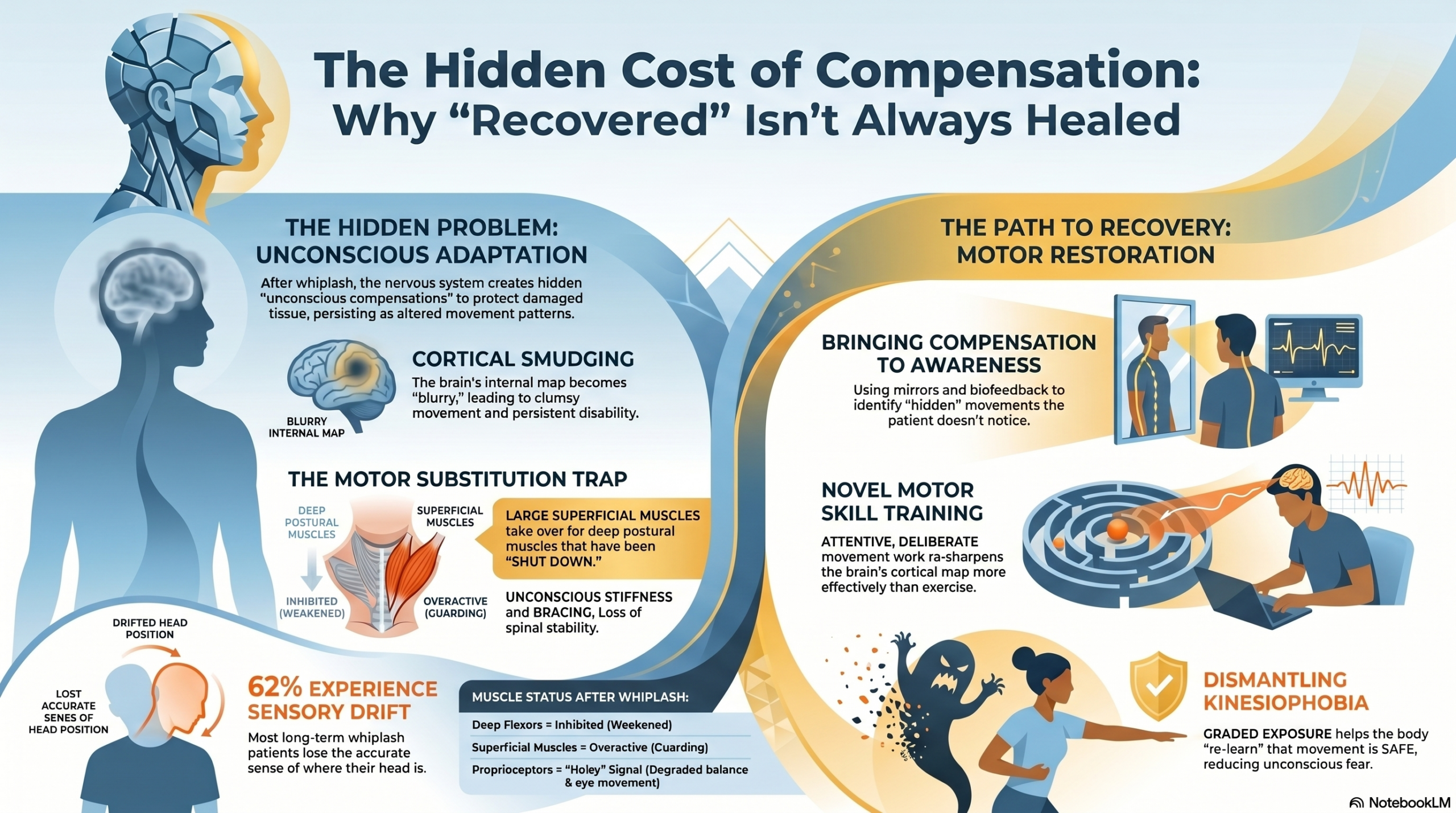
After a whiplash injury, three things change in the way you move, and you almost certainly will not notice any of them.
The first is guarding. Guarding is the protective behavior your nervous system installs to keep you from re-injuring tissue that is — or recently was — damaged. It looks like stiffness, hesitation, bracing, and avoidance of certain ranges of motion. It feels like nothing. You don’t feel guarded; you just feel “normal,” because your normal has been quietly redrawn around the injury. The literature on chronic pain has spent decades trying to characterize guarding precisely, and the most consistent finding is that it persists long after the original tissue has healed and is largely independent of current pain intensity.
The second is altered motor control. This one is more subtle and more consequential. The deep, postural muscles of your neck — small muscles called the longus colli and longus capitis that sit deep against the front of your spine and act like the rigging that holds a sailboat’s mast steady — get inhibited after a whiplash. Inhibited means: the brain stops recruiting them properly. In their place, the big superficial muscles you can feel from the outside — the sternocleidomastoid, the upper trapezius, the scalenes — take over jobs they were never designed to do. You move your head, but you do it with the wrong machinery. From the outside it looks the same. From the inside, the motor strategy has been reshuffled.
The third is proprioceptive drift. Your neck contains an extraordinary density of position sensors — receptors in the joints, ligaments, and especially the deep suboccipital muscles between your skull and your top vertebrae — that tell your brain in real time where your head is in space. After whiplash, those sensors get noisy. The signal degrades. Your brain’s internal map of your neck becomes blurry. You might pass every test your primary care doctor knows how to administer, but your sense of where your head is is measurably less accurate than it was before the crash. You don’t feel that. You feel like your head is exactly where you think it is.
Stack these three changes together — guarding, altered motor recruitment, and proprioceptive drift — and you have a person whose movement patterns have been rewritten without their consent and below their notice. James, in his car, wasn’t choosing to swivel his whole body. His brain had quietly shut down the rotation his neck used to perform and substituted a torso turn. His brain considered this a successful solution. He considered it normal.
The compensation works, in the short term. That’s what makes it so dangerous. It successfully gets your head turned. It successfully gets your eyes onto the rear-view mirror. It successfully gets your hand to the cup of coffee. The cost — joint loading distributed onto regions that weren’t designed for it, muscles working at the wrong intensity, posture pulled subtly out of alignment — is invoiced months or years later, in a different region of the body, and almost no one connects it back to the crash.
A successful compensation is one your body bills you for later. The bill comes in a different envelope than the original injury, which is why most people never figure out what they’re paying for.

The Research: Five Categories of Evidence
The phenomenon I’m describing isn’t speculation. It’s one of the most consistently documented findings in the entire whiplash literature. Let me walk you through what the research has shown across five categories, each with the PMID so you can read the studies yourself.
1. Altered motor control after whiplash is real, measurable, and persistent
A foundational study by Woodhouse and Vasseljen looked at neck movement patterns in chronic whiplash patients, chronic non-traumatic neck pain patients, and healthy controls. They found altered motor control strategies in both pain groups — strategies that did not normalize even when pain was low. The changes in movement were not strictly tied to current pain levels but appeared to be driven by long-lasting changes in how the central nervous system organized neck movement.
Research
PMID 18570647 — Woodhouse A, Vasseljen O. BMC Musculoskelet Disord. 2008. Altered motor control patterns documented in both whiplash and chronic neck pain groups. Changes persisted independent of current pain levels, indicating long-lasting motor reorganization rather than simple pain-driven guarding.
A 2017 systematic review by Stenneberg and colleagues looked specifically at cervical motor dysfunction in patients with whiplash and asked whether early dysfunctions could predict who would still be symptomatic a year later. Reduced active range of motion was a predictive factor for chronic disability. How your motor control looks in the first six weeks tells us a great deal about where you’ll be twelve months out.
Research
PMID 28522239 — Stenneberg MS et al. Arch Phys Med Rehabil. 2017. Reduced cervical mobility, disturbed kinaesthesia, and altered muscle activity were established early predictors of chronic disability in whiplash-associated disorders.
2. Deep neck flexors get inhibited and don’t come back on their own
The deep cervical flexors are the small, postural muscles I mentioned earlier — the ones that hold the cervical spine stable while the bigger muscles do the heavy work. Gwendolen Jull and Deborah Falla, two of the most important researchers in this field, have spent careers showing that these muscles get inhibited after both whiplash and insidious-onset neck pain.
In a 2004 study, Jull’s group compared whiplash patients to people with non-traumatic chronic neck pain on a clinical test called the craniocervical flexion test. Both pain groups showed measurably reduced deep cervical flexor performance. The researchers also found that patients compensated by recruiting their superficial sternocleidomastoid muscles more — exactly the substitution pattern I described above.
Research
PMID 15040968 — Jull G, Kristjansson E, Dall’Alba P. Man Ther. 2004. Whiplash and insidious-onset neck pain patients both demonstrated impairment of the deep cervical flexor muscles, with compensatory overactivity of the superficial sternocleidomastoid. The dysfunction was not self-correcting.
A separate study from Falla’s lab measured electromyographic activity directly during the craniocervical flexion test and confirmed the finding: patients with neck pain showed reduced activation of the deep cervical flexors and increased activation of the superficial neck flexors. The body had reassigned the work to the wrong department.
Research
PMID 15454700 — Falla DL, Jull GA, Hodges PW. Spine. 2004. EMG evidence of reduced deep cervical flexor activity and increased superficial flexor activity during the craniocervical flexion test in patients with chronic neck pain — the precise motor substitution pattern that defines unconscious compensation.
3. Proprioception — your sense of where your head is — gets measurably worse
In 1997, Loudon and colleagues asked whiplash patients and matched controls to close their eyes and reproduce a target head position. The whiplash patients consistently missed. They couldn’t put their heads back where they thought they were putting them, with statistically significant deficits compared to uninjured controls.
Research
PMID 9127919 — Loudon JK, Ruhl M, Field E. Spine. 1997. Whiplash patients showed significant deficits in their ability to reproduce a target head position with eyes closed, indicating altered cervical proprioceptive accuracy after injury.
A subsequent study by Treleaven and colleagues took the same idea further and connected the proprioceptive deficit to balance disturbances and abnormal eye movements in persistent whiplash. The researchers found that 62% of patients with whiplash trauma greater than two years had repositioning dysfunction and pathologic oculomotor testing. The neck wasn’t just stiff. Its connection to the entire visual-vestibular-postural system was degraded.
Research
PMID 15919229 — Treleaven J, Jull G, Sterling M. J Rehabil Med. 2003. Cervical joint position error correlated with balance and oculomotor dysfunction in persistent whiplash. The neck’s role as a proprioceptive sense organ for the entire postural system is compromised by injury.
4. The motor cortex itself gets reorganized — and the reorganization tracks the pain
The most striking finding comes from imaging studies of the brain itself. Tsao and colleagues, in a 2011 study that won an ISSLS prize, used transcranial magnetic stimulation to map the motor cortical representation of the back muscles in young adults with recurrent low back pain. They found that the cortical map had become “smudged” — the discrete representations of individual muscles had merged into an indistinct blur. The smudging correlated with the severity of the pain.
The phenomenon isn’t unique to the back. The same kind of cortical disorganization has been documented in chronic neck pain. The brain stops being able to address its individual muscles as separate addresses and begins firing them in clumps.
Research
PMID 21508892 — Tsao H, Galea MP, Hodges PW. Eur Spine J. 2011. ISSLS prize-winning study demonstrating “smudging” of motor cortex representations in chronic back pain. Discrete muscle representations merge into indistinct cortical regions, and the degree of smudging correlates with pain severity.
A complementary line of work by Lorimer Moseley and colleagues showed that chronic back pain patients couldn’t accurately delineate the outline of their own back when asked to draw it from internal sense alone. Two-point discrimination — the ability to feel two distinct points of touch on the skin as separate — was significantly degraded in the painful region. The brain had lost some of its representational fidelity for the part of the body that hurt.
Research
PMID 18786763 — Moseley GL. Pain. 2008. Chronic back pain patients showed disrupted internal body image of the affected region, with degraded two-point discrimination. The brain’s map of the painful body part literally becomes less detailed.
5. Fear of movement — kinesiophobia — quietly drives the whole thing
A network analysis published in 2023 found that fear of movement was one of the strongest predictors of headache and neck pain intensity and disability in people with whiplash-associated disorders, both in the acute phase and at six-month follow-up. The kinesiophobia is unconscious in the same way the guarding is unconscious. Patients don’t consciously decide to be afraid of turning their head. The fear is encoded somatically — as a flinch, as a brake, as a “no thanks” reflex when the brain considers a particular movement.
Research
PMID 37725095 — De Pauw R et al. Eur J Pain. 2023. Fear of movement was strongly associated with headache, neck pain intensity, and disability in WAD patients at both acute and six-month timepoints. Fear of movement is not a downstream consequence — it is one of the structural drivers of persistent disability.
The Deeper Science: Why Unconscious Compensation Is the Default
To understand why your body adapts without telling you, it helps to understand a basic principle of how your nervous system handles injury.
When tissue is damaged, the brain’s first priority is not to record the experience for later analysis. Its first priority is to keep you functional and alive. It floods the injured region with inflammatory chemistry that produces pain — pain that is a signal, not the injury itself. And it begins, instantly, to construct a new motor strategy that lets you keep moving despite the damage.
This new strategy gets installed at the level of the motor cortex and the brainstem — below the level of conscious choice. Consciousness sits in the prefrontal cortex; motor strategy sits much deeper. By the time you become aware of how you’re moving differently, your basal ganglia and cerebellum have already rewritten the program.
This is, evolutionarily, a beautiful system. If a saber-toothed tiger has clawed your shoulder, you do not want to spend cognitive bandwidth re-learning how to throw a spear. You want your nervous system to figure out a workaround in the background while your prefrontal cortex stays focused on not getting eaten. The unconscious compensation system is what kept our ancestors alive.
The problem is that the system was designed for a world where injuries either killed you or healed quickly and completely. In modern life — particularly in the world of low-velocity collisions where soft tissue is sprained, ligaments are stretched, and proprioceptors are damaged but bone is intact — the injury heals partially or imperfectly, and the compensation persists. The motor strategy that was supposed to be temporary becomes permanent. The neural map that was supposed to remap as soon as the tissue healed never quite remaps, because the smudging of the cortical representation is itself self-reinforcing. A blurry map produces clumsy movement, clumsy movement produces continued threat signaling, continued threat signaling further blurs the map.
This is the loop that turns an acute whiplash into a chronic pain syndrome. And the most important insight from the last twenty years of motor learning research is that the loop will not unwind by itself. Pain reduction is not the same as motor restoration. You can be pain-free and still be moving with a fundamentally compromised strategy that will eventually generate new pain in a new region.
This is why James, fourteen months out, with no acute neck pain, was developing aching shoulders, a tight low back, hip pain when he ran, and intermittent headaches. The acute injury had healed. The compensation hadn’t.
Pain reduction is not the same as motor restoration. The first is the alarm turning off. The second is the actual repair of how you move. They are not the same job, and neither one does the other’s work.

What Bringing Compensation to Awareness Actually Looks Like in Clinic
Awareness, in this context, is not a vague mindfulness platitude. It’s a specific clinical process with specific steps. Here’s what a session in our Petaluma clinic actually looks like when we’re doing this work.
Step one: I watch you move. Before I touch you, before I take a history, before I send you for any test, I watch you walk to the treatment room, sit down, take off your jacket, look at your phone. I am cataloguing the compensations you don’t know you’re making. Asymmetric arm swing. A head that always turns to the same side first. A subtle rotation of the trunk when you shift your gaze. A jaw that clenches on side bend. None of this is in the diagnostic codes. All of it is in the body.
Step two: I make you watch yourself move. This is the part most patients have never done. We use a mirror, sometimes a video on a tablet, sometimes a simple verbal cue — “as you turn your head, tell me what you notice.” The first thing patients almost always say is “huh — I didn’t know I did that.” That sentence, “I didn’t know I did that,” is the beginning of awareness. Until you’ve heard yourself say it, the compensation lives in a region of your nervous system you cannot reach.
Step three: I find your deep cervical flexors and ask you to re-introduce yourself to them. I use a pressure biofeedback unit, a small inflatable cuff placed behind the neck that lets you and I both see — in real-time, as a number on a gauge — whether you are gently nodding your chin using the deep flexors or whether you are jamming your head down using the big superficial muscles. Almost no patient gets this right on the first attempt. By the third or fourth visit, most patients can find the muscles. By the eighth or tenth visit, the muscles can begin to take their proper place in everyday movement.
Step four: I retrain your sense of where your head is. This is direct proprioceptive rehabilitation. You sit, eyes closed, I move your head to a target position. You open your eyes, see where it is, close your eyes, and try to return to that position from a new starting point. We measure the error. We work with it. Across sessions, the error shrinks. The cervical map gets sharper.
Step five: I ask you to expand the menu. This is the part of the process most directly aimed at unconscious avoidance. I ask you to do the movements you have stopped doing — slowly, gradually, with my hands available if needed, in graded exposure. Looking up. Looking sharply over each shoulder. Tilting the ear toward the shoulder. Rotation under load. The brain starts adding these movements back to the menu. Kinesiophobia is dismantled not by a conversation but by the body discovering, repetition by repetition, that the movement is safe.
Step six: I teach you to monitor at home. Every patient who comes through this protocol leaves with two or three “awareness checkpoints” they can run during the day. How does my breath feel right now? Where is my chin? Am I turning with my whole body or with my neck? These are not exercises. They are check-ins. They install a habit of perception that, over time, replaces the unconscious compensation with a conscious option to move differently.
A typical course of care runs eight to twelve weeks for a patient who is six to twelve months out from injury. Patients further out — like James, more than a year — sometimes need longer, because the compensations have had more time to embed. The work is not glamorous. It is detailed. It is repetitive. And it produces durable change in a way that no passive treatment, no medication, and no scan can produce.
The research on motor learning in chronic musculoskeletal pain backs this up directly. Boudreau and colleagues, in a foundational 2010 paper, argued that novel motor skill training — exactly the kind of attentive, deliberate movement work I just described — produces measurable cortical reorganization in the direction of recovery, in a way that simple repetition of general exercise does not.
Research
PMID 20615749 — Boudreau SA, Farina D, Falla D. Man Ther. 2010. Novel motor-skill training drives cortical reorganization and improves task performance in musculoskeletal pain populations — in contrast to passive treatment or general exercise. The cortical map can be re-sharpened, but only by the right kind of practice.
The mindfulness and body-awareness literature converges on the same point from a different direction. A 2017 systematic review and meta-analysis of mindfulness-based interventions for chronic pain, covering thirty randomized controlled trials, found small but consistent improvements in pain symptoms and high-quality evidence for improvement in depression and quality of life. The mechanism — sustained, directed attention to bodily sensation — is, at the neuroscience level, the same mechanism by which cortical maps re-sharpen.
Research
PMID 27658913 — Hilton L, Hempel S, Ewing BA, et al. Ann Behav Med. 2017. Meta-analysis of 30 RCTs showed mindfulness-based interventions produced statistically significant improvements in pain, depression, and quality of life. The shared mechanism with motor rehabilitation is directed attention to the body — the antidote to unconscious adaptation.
The Takeaway
If you’ve been in a collision in the last year or two, here is what I want you to take from this article.
The fact that your acute neck pain has resolved does not mean the compensation has resolved. The fact that you feel like you’re moving normally does not mean you’re moving normally. Your body has been quietly editing its motor strategy in the background since the moment of impact, and the edits, untreated, become the chronic syndrome that shows up later as shoulder pain, low back pain, headache, balance problems, or dizziness.
You are not crazy if you sense that “something hasn’t been quite right since the accident” even when no scan shows anything and no doctor can find anything. The mismatch between how the medical system measures recovery and what your nervous system is actually doing is exactly the mismatch this article is about. The system measures pain. Your nervous system has moved on to compensation. Those are different problems with different solutions.
The most important thing you can do is get evaluated by a clinician who treats movement as the primary diagnostic data — not as something secondary to imaging. If your evaluator can run a craniocervical flexion test, measure your joint position error, watch you move and tell you something specific about how your motor strategy has changed, and build a graded re-training protocol around those findings, you are in the right hands. If they look at a scan, tell you it’s normal, and send you home, you are not in the wrong hands so much as in the wrong specialty.
What to Do Now
If you’ve been in a crash in the last twenty-four months and you’ve noticed that you “just don’t move the same anymore” — book a movement-based evaluation. Not because the change feels dramatic, but because the silent compensations are exactly the ones that turn into chronic syndromes if left unaddressed. In our Petaluma clinic this is core work, every day.
You don’t have to live with adaptations you didn’t agree to. The body that learned to compensate without your awareness can re-learn to move with your awareness. The catch — and there is a catch — is that the re-learning is not automatic. It requires somebody who knows what to look for, the right tools to measure it, and a patient willing to do the slow, attentive work of meeting their own body again.
James, the patient I started this article with, came back for his twelve-week follow-up and told me he’d caught himself looking over his shoulder for the first time in over a year. Not because he’d thought about it. Because he’d done it before noticing he’d done it. The compensation had finally been replaced by the original movement. That moment — when the right movement returns to the unconscious menu — is what we’re working toward. It is not a small moment. It is, in fact, the moment recovery actually finishes.
You don’t have to spend the next decade of your life paying compensations on a debt you didn’t know you owed.
References
- Woodhouse A, Vasseljen O. Altered motor control patterns in whiplash and chronic neck pain. BMC Musculoskelet Disord. 2008. PMID 18570647.
- Stenneberg MS, Rood M, de Bie R, et al. Active cervical range of motion in patients with neck pain, whiplash, and controls: A systematic review and meta-analysis. Arch Phys Med Rehabil. 2017. PMID 28522239.
- Jull G, Kristjansson E, Dall’Alba P. Impairment in the cervical flexors: a comparison of whiplash and insidious onset neck pain patients. Man Ther. 2004. PMID 15040968.
- Falla DL, Jull GA, Hodges PW. Patients with neck pain demonstrate reduced electromyographic activity of the deep cervical flexor muscles during performance of the craniocervical flexion test. Spine. 2004. PMID 15454700.
- Loudon JK, Ruhl M, Field E. Ability to reproduce head position after whiplash injury. Spine. 1997. PMID 9127919.
- Treleaven J, Jull G, Sterling M. Dizziness and unsteadiness following whiplash injury. J Rehabil Med. 2003. PMID 15919229.
- Tsao H, Galea MP, Hodges PW. Smudging the motor brain in young adults with recurrent low back pain. Eur Spine J. 2011. PMID 21508892.
- Moseley GL. I can’t find it! Distorted body image and tactile dysfunction in patients with chronic back pain. Pain. 2008. PMID 18786763.
- De Pauw R, Coppieters I, Caeyenberghs K, et al. Network analyses on fear of movement and neck pain in WAD. Eur J Pain. 2023. PMID 37725095.
- Boudreau SA, Farina D, Falla D. Motor learning and neuroplasticity in musculoskeletal pain. Man Ther. 2010. PMID 20615749.
- Hilton L, Hempel S, Ewing BA, et al. Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-analysis. Ann Behav Med. 2017. PMID 27658913.
- Lundberg M, Grimby-Ekman A, Verbunt J, Simmonds MJ. Pain-related fear: a critical review of the related measures. Pain Res Treat. 2011. PMID 21886284.
