Blurring Specialties — Why Whiplash Demands More Than One Kind of Doctor
She came in holding her neck, but that wasn’t the real problem.
Sarah sat across from me in my office at Adjust Clinic, one hand cradling her cervical spine like it might shatter. Three months earlier, a rear-impact collision at a red light had sent her forward and backward in what felt like a split second. The emergency room had cleared her imaging—no fracture, no dislocation—and sent her home with muscle relaxants and a prescription pad full of reassurance. You’ll be fine in a few weeks. That’s what they’d told her.
But Sarah wasn’t fine. The neck pain was real enough, but it was almost the least of it. What kept her up at night was the fog. The sensation that her thoughts were moving through water. She’d lose her train mid-sentence. She’d read a paragraph and have no memory of it. She felt dizzy when she turned her head, and worse—anxious. Panicked, even. Her heart would race. She’d have this terrible sense of impending doom for no reason at all, then it would pass, leaving her exhausted.
She’d been to three doctors. One orthopedist had done some imaging and prescribed physical therapy for her neck. A neurologist had ruled out a concussion and essentially shrugged. A psychiatrist had suggested anxiety medication. Everyone was talking about a different patient.
“I feel like I’m falling apart,” she told me, “but nobody’s looking at the whole picture.”
That’s when I realized: Sarah wasn’t the problem. The system was.
The Anatomy of a Misunderstanding
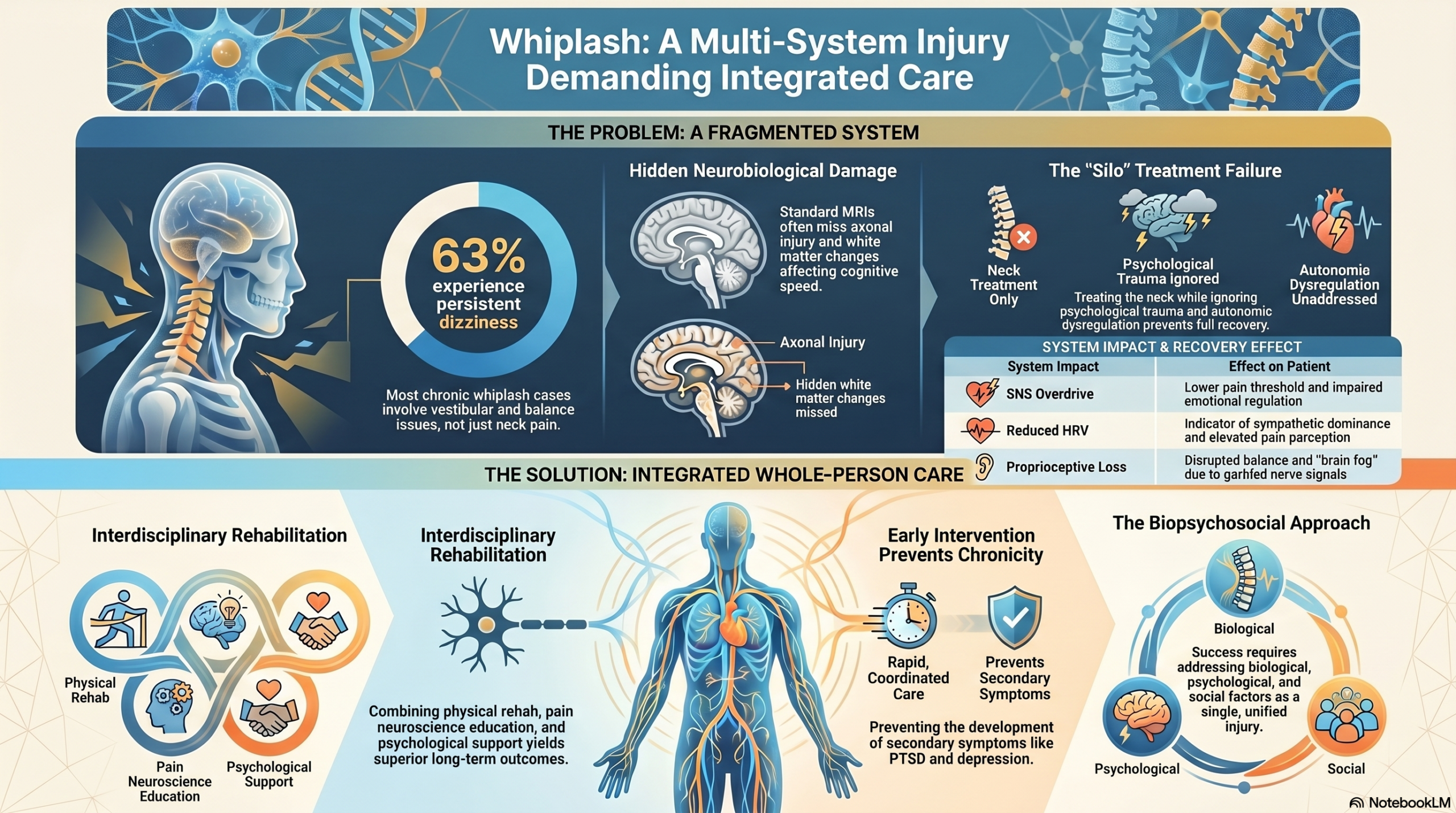
Here’s what most people—and frankly, many healthcare providers—don’t understand about whiplash: it’s not just a neck injury. The cervical spine isn’t a separate body part that works in isolation. It’s one of the most densely innervated regions of the human body, a crossroads where orthopedic, neurological, vestibular, and autonomic systems intersect. Damage that whiplash causes doesn’t respect disciplinary boundaries. It can’t be adequately treated by one kind of doctor because the injury itself doesn’t fit into one medical specialty.
When I was training, I was taught a very linear model: whiplash damages soft tissue in the neck, which causes pain, which gets treated with rest and rehabilitation. Simple. Clean. Wrong.
The cervical spine contains roughly 600 proprioceptive nerve endings per gram of tissue in the facet joints and neck muscles—more concentrated sensory apparatus per cubic centimeter than almost anywhere else in the body. These proprioceptors aren’t just reporting on the position of your neck. They’re feeding constant information to your vestibular system, your visual system, your balance centers, and to areas of your brain involved in mood regulation and cognition.
When whiplash happens, it doesn’t just stretch muscles. It can disrupt these proprioceptive pathways. It can trigger inflammatory cascades that sensitize the nervous system. It can dysregulate the autonomic nervous system—the system responsible for your heart rate, breathing, digestion, and threat-detection mechanisms. It can damage axons in ways that aren’t visible on an MRI but show up on advanced imaging like diffusion tensor imaging. All of this happens simultaneously.
And yet, most patients see a chiropractor or physical therapist focused on the mechanical problem, or an orthopedist who largely ignores the neurological and psychological sequelae, or a psychiatrist treating depression and anxiety as if they exist in a vacuum, separate from the body that was just traumatized.
This is how Sarah ended up fragmented across three doctors, each treating a different symptom while missing the unified injury underneath.

The Case for Integration: What the Research Actually Shows
I want to take you through the evidence systematically, because this isn’t philosophy or preference. This is science telling us that whiplash is fundamentally multi-system, and single-specialty treatment is inadequate.
Vestibular and Proprioceptive Dysfunction: The Dizziness Problem
Let’s start with something Sarah experienced acutely: dizziness. She described it as a sensation of spinning when she turned her head, or sometimes a floating feeling, as if the world was slightly tilted.
Your neck proprioceptors send signals up to your brainstem, to a cluster of neurons called the vestibular nuclei. These nuclei integrate information from your neck, your eyes, and your inner ear to create a coherent sense of where your head is in space and how fast it’s moving. When the cervical spine is injured, the proprioceptive input becomes garbled. Your brainstem gets conflicting signals: the neck is saying one thing, the inner ear another, your eyes something else. The result is dizziness, imbalance, and sometimes nausea.
Research Evidence: Balance and Dizziness in Whiplash
Study: Dizziness, balance problems, and proprioceptive disturbance in chronic whiplash-associated disorders (WAD)
Finding: 63% of patients with chronic whiplash had persistent dizziness and balance disturbances; these symptoms were associated with proprioceptive deficits in the neck, not just pain.
Source: PMID 26678652
Research Evidence: Cervicogenic Dizziness Diagnosis
Study: Diagnostic criteria and mechanisms of cervicogenic dizziness
Finding: Whiplash frequently causes mismatch between cervical proprioceptive, vestibular, and visual inputs at the vestibular nuclei level, requiring specialized assessment.
Source: PMC 5759906
Here’s the critical point: you can’t treat this with neck pain medications alone. You need vestibular rehabilitation. You need proprioceptive retraining. You need someone who understands the relationship between cervical mechanoreceptors and balance.
Psychiatric and Psychological Sequelae: The Anxiety That Follows
Sarah’s anxiety was also being treated in isolation. Whiplash is a trauma—an unpredictable, sudden assault on the body. Even if there’s no serious structural injury, the brain registers it as threat. In some patients, this activates persistent changes in how the threat-detection system operates. The amygdala becomes hypersensitive. The prefrontal cortex becomes less effective at inhibiting it.
Add to that the fact that the autonomic nervous system is already dysregulated from the injury itself, and you get a perfect storm: a nervous system primed to detect threat, and a body that feels unsafe.
Research Evidence: Psychiatric Outcomes After Whiplash
Study: Systematic review of psychiatric sequelae following whiplash injury
Finding: Whiplash patients show elevated rates of PTSD, major depression, and anxiety disorders; these persist in 30–50% of chronic cases and involve neurobiological sensitization.
Source: PMID 35530017
Research Evidence: Psychological Factors Predicting Chronicity
Study: Psychological factors and recovery expectations in chronic whiplash-associated disorders
Finding: Poor recovery expectations, PTSD symptoms, and passive coping strategies at baseline predict development of chronic pain; these are modifiable factors that respond to psychological intervention.
Source: PMID 29470185
Cognitive Symptoms: The Brain Fog That Lingers
Sarah described her cognitive fog as the most disabling symptom. It was affecting her work. Brain fog after whiplash isn’t a psychiatric symptom—it’s a neurobiological change.
Whiplash can cause traumatic axonal injury (TAI)—subtle damage to the long nerve fibers that transmit information throughout the brain. It’s not visible on standard MRI, but it shows up on diffusion tensor imaging (DTI).
Research Evidence: Traumatic Axonal Injury in Whiplash
Study: Diffusion tensor imaging reveals white matter changes and traumatic axonal injury in whiplash-associated disorders
Finding: Patients with chronic whiplash show significant white matter abnormalities on DTI; these correlate with cognitive complaints including memory deficits, processing speed reduction, and concentration problems.
Source: PMC 5809420
Autonomic Dysregulation: The Nervous System in Overdrive
Here’s where everything connects. Your autonomic nervous system has two main branches: the sympathetic (gas pedal) and parasympathetic (brake pedal). When you’re in a chronic state of sympathetic overdrive, your pain threshold drops, your sensitivity to sensory input increases, and your emotional regulation becomes impaired.
Research Evidence: Heart Rate Variability and Pain in Whiplash
Study: Lower heart rate variability (HRV) relates to high pain catastrophizing in chronic WAD
Finding: Reduced HRV—an indicator of parasympathetic withdrawal and sympathetic dominance—is associated with elevated pain perception and maladaptive pain cognitions.
Source: PMID 26614574
Research Evidence: Sympathetic Nervous System Effects on Sensorimotor Function
Study: Influence of sympathetic nervous system on sensorimotor function in WAD
Finding: Sympathetic activation impairs proprioceptive acuity, increases pain sensitivity, and disrupts motor control—creating a self-reinforcing cycle.
Source: PMID 17036216
Research Evidence: Resting Physiology and Pain Processing
Study: Associations between resting heart rate, blood pressure, psychological variables, and pain processing in chronic whiplash
Finding: Elevated baseline heart rate and blood pressure, reflecting sympathetic overactivation, correlate with enhanced pain processing, anxiety, and depression.
Source: PMC 9629357
The Integrated Biopsychosocial Model: Putting It Together
So we have proprioceptive dysfunction driving vestibular and cognitive symptoms. We have trauma and autonomic dysregulation driving anxiety and mood changes. We have inflammatory cascades and axonal injury driving pain and fatigue. These aren’t separate problems. They’re facets of a single integrated injury.
Research Evidence: Sterling’s Integrated Model of Chronic Whiplash
Study: Whiplash-associated disorders: Psychological and neurobiological factors in chronic pain and disability
Finding: Chronic whiplash results from interaction between peripheral sensory dysfunction, altered central pain processing, and psychological factors; changes in any one component influence the others.
Source: PMID 28622487
Research Evidence: The Biopsychosocial Approach to Chronic Pain
Study: Biopsychosocial approach to understanding chronic pain and disability
Finding: Chronic pain conditions respond better to treatment when biological, psychological, and social factors are addressed in an integrated manner.
Source: PMID 17592957
“If you’re treating only the neck, you’re leaving 70% of the problem untouched.”
The Neuroscience of a Grand Central Station
The cervical spine is extraordinarily rich in sensory innervation. The facet joints, the muscles, the ligaments—they’re all packed with proprioceptive mechanoreceptors. This information travels up to the brainstem, where it converges with vestibular information and visual information to create a unified sense of spatial orientation and movement.
From the brainstem, this integrated sensory information relays through the thalamus to the cortex—to the sensorimotor cortex, the insular cortex, and the prefrontal cortex.
When whiplash happens, it disrupts this entire pipeline. The thalamus becomes sensitized and passes through more signals, more intensely, than it normally would. This creates central sensitization—the nervous system becomes hypersensitive to sensory input and misinterprets non-threatening signals as threatening.
Meanwhile, the autonomic dysregulation creates a feedback loop. Sympathetic activation impairs proprioceptive acuity—the very receptors you need to recover become less effective—which means the proprioceptive dysfunction persists, maintaining the threat signals that keep the sympathetic system engaged.
This is why whiplash patients often feel trapped. The system becomes self-sustaining.

What Integrated Care Actually Looks Like
When Sarah came to Adjust Clinic, we did something different. We treated her as a whole system.
We looked at her vestibular function, assessed proprioceptive acuity, screened for cognitive deficits, did autonomic assessment including heart rate variability measurement, and listened to her psychological experience.
The chiropractic component focused on restoring normal cervical mechanics and proprioceptive signaling. We paired this with vestibular rehabilitation—gaze stability exercises, habituation exercises, balance retraining. We included pain neuroscience education. We coordinated psychological support with a trauma-informed therapist. We addressed autonomic dysregulation through vagal toning exercises, breathing work, and lifestyle modifications.
Critically, all of these pieces were coordinated. My team communicated with her physical therapist and her therapist.
Research Evidence: Interdisciplinary Rehabilitation Outcomes
Study: Five-year outcomes of interdisciplinary rehabilitation program for WAD
Finding: Interdisciplinary programs combining physical rehabilitation, pain neuroscience education, psychological treatment, and coordinated care achieve better long-term functional outcomes and lower disability rates.
Source: PMID 28248865
Research Evidence: Early Interdisciplinary Intervention
Study: Early interdisciplinary rehabilitation programme following whiplash injury
Finding: Early interdisciplinary treatment reduces chronicity rates and prevents development of secondary psychological symptoms.
Source: PMID 11400904
Over twelve weeks, Sarah’s trajectory shifted. By three months, she was back at work. By six months, the symptoms were background noise. By a year, she felt like herself again.
A Whole Person Needs Whole Care
Your whiplash injury isn’t just an orthopedic problem, a neurological problem, or a psychological problem. It’s a whole-body, whole-system disruption that demands a whole-person response.
If you’ve experienced whiplash and have felt like you’re falling apart—like different doctors are treating different pieces while the central problem remains—you’re not crazy. The system has been fragmented. You need integration.
At Adjust Clinic, we specialize in exactly this. We’ve built a practice around the recognition that whiplash is multi-system, that recovery requires integration, and that patients deserve more than the current fragmented standard.
If that resonates, I’d invite you to schedule an evaluation. We’ll do a thorough assessment of your entire system—not just your neck. We’ll explain what we find in plain language. And we’ll build a coordinated treatment plan that actually addresses the whole problem.
“A whole person needs whole care. You deserve that. Your nervous system deserves that. Let’s get you there.”
References
- Dizziness, balance problems, and proprioceptive disturbance in chronic whiplash-associated disorders — PMID 26678652
- Diagnostic criteria and mechanisms of cervicogenic dizziness — PMC 5759906
- Psychiatric sequelae following whiplash injury: Systematic review — PMID 35530017
- Psychological factors and recovery expectations in chronic WAD — PMID 29470185
- Diffusion tensor imaging reveals white matter changes in WAD — PMC 5809420
- Lower heart rate variability relates to high pain catastrophizing in chronic WAD — PMID 26614574
- Influence of sympathetic nervous system on sensorimotor function in WAD — PMID 17036216
- Associations between resting heart rate, blood pressure, psychological variables, and pain processing in chronic whiplash — PMC 9629357
- Whiplash-associated disorders: Psychological and neurobiological factors — PMID 28622487
- Biopsychosocial approach to understanding chronic pain and disability — PMID 17592957
- Five-year outcomes of interdisciplinary rehabilitation program for WAD — PMID 28248865
- Early interdisciplinary rehabilitation programme following whiplash injury — PMID 11400904
This article is for educational purposes. If you have experienced a motor vehicle accident or whiplash injury, consult a qualified healthcare provider for evaluation and treatment specific to your situation.
Adjust Clinic — Sonoma County Personal Injury Chiropractic
