Bodies Remember What Minds Forget
How the nervous system archives trauma long after the mind has moved on—and what it means for your recovery from whiplash.
Introduction: The Crash You’ve Already Processed
Think back to the moment of impact. A fraction of a second. The sound—metallic, sudden, wrong. Then stillness, and the slow inventory: Am I okay?
For most people, the answer in those first minutes seems to be yes. The car is drivable. You declined the ambulance. You gave a statement, exchanged insurance cards, and drove home. By the time you poured yourself a glass of water that evening, you had already begun the psychological work of filing the experience away. You processed it. You moved on.
Your nervous system did not.
In twenty-five years of chiropractic practice—and across more than a thousand personal injury cases treated in Sonoma County in the past four years alone—I keep encountering the same patient. They arrive weeks, sometimes months, after a collision they themselves describe as “minor.” The car damage was modest. The ER found nothing on imaging. They were told to rest, take ibuprofen, and expect to feel better within two weeks. They didn’t.
I know what you might be thinking: If there’s nothing on the scan, how can there still be something wrong?
Here’s what’s actually happening. The body is not a machine that either breaks or doesn’t. It is an archive—a living, adaptive record of every force it has absorbed and every threat it has detected. Long after the mind has cognitively processed a car accident as a closed chapter, the spine, the nervous system, and the deep proprioceptive networks of the body continue operating under altered protocols. They are still, in a very real neurological sense, on guard.
This essay is about why that happens, what the science says, and why understanding it changes everything about how we approach recovery from whiplash and soft-tissue collision injuries.
Section 1: The Biomechanics of Impact—What Happens in the 300 Milliseconds You Cannot Remember

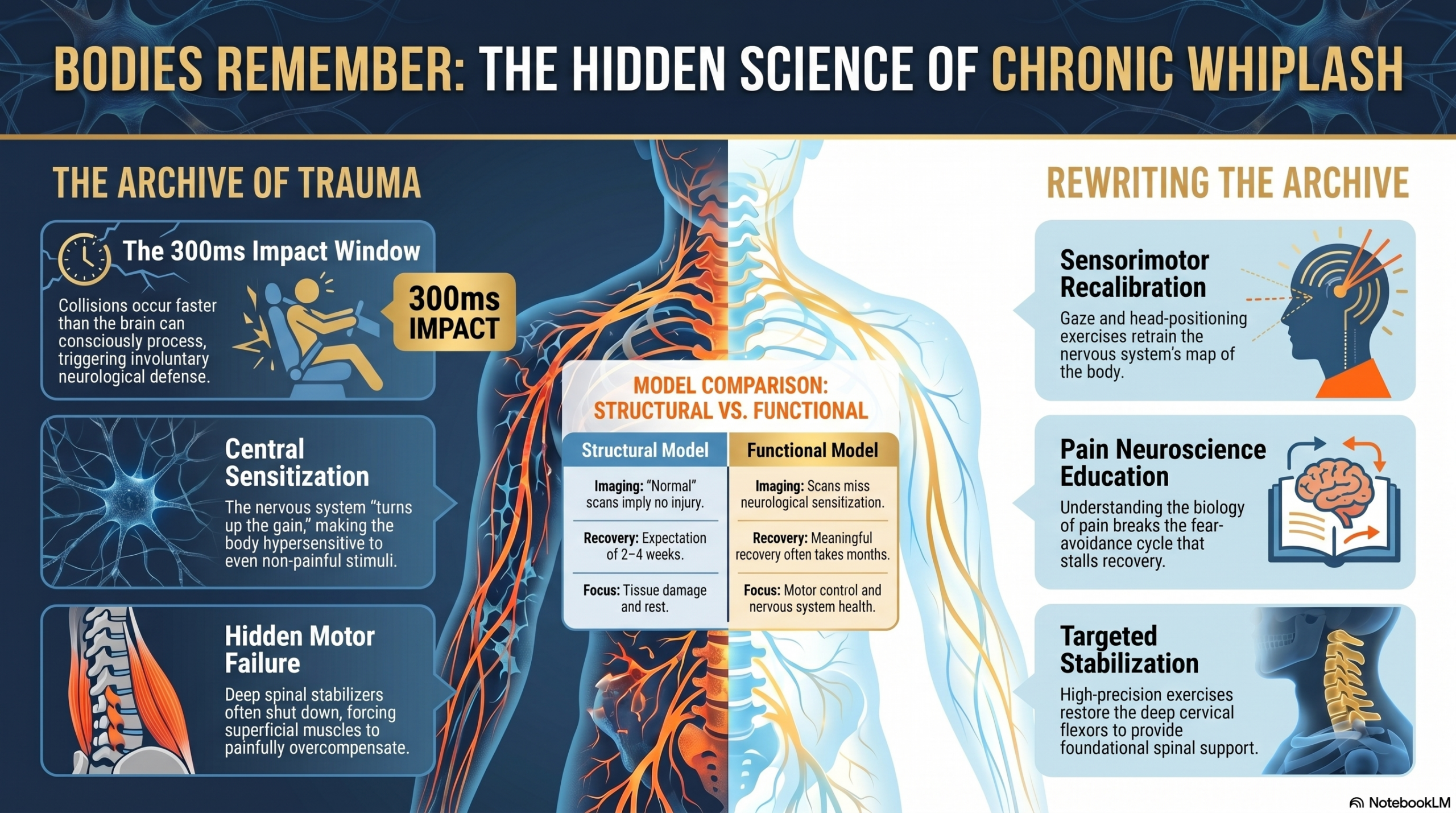
The human brain can process a visual stimulus in roughly 250 milliseconds. A rear-end collision—even at low speed—can complete its full biomechanical cycle in as little as 150 to 300 milliseconds. You cannot consciously perceive the event before your body has already been stressed by it.
This is not a trivial detail. It carries profound clinical consequences.
In the classic rear-end whiplash event, the torso is accelerated forward by the seat while the head—unsupported in space—lags behind momentarily, then snaps forward through a complex S-shaped curve. This creates a two-phase injury mechanism: first, a hyperextension phase where the lower cervical segments move into unnatural extension while the upper segments paradoxically flex; then a rebound hyperflexion phase as the head snaps forward. The ligaments, facet joint capsules, intervertebral discs, and deep paraspinal muscles are all subjected to rapid tensile and compressive forces through both phases.
What makes this biomechanically significant is that the forces generated at the cervical spine can exceed the tissue injury threshold even at collision speeds that produce minimal visible vehicle damage. Research published in the Journal of Biomechanics has consistently demonstrated that low-speed impacts of 8 to 10 mph can generate cervical acceleration forces sufficient to strain soft tissues—because vehicle deformation is itself a form of energy absorption. A stiffer bumper transfers more force to the occupant. Low damage to the car and high stress to the body are not contradictory; they are sometimes causally related.
And here is what imaging almost never captures: the body’s response to this rapid, involuntary motion is not purely mechanical. It is neurological. Within milliseconds of impact, proprioceptors in the facet joint capsules, muscle spindles in the deep cervical musculature, and mechanoreceptors throughout the cervical connective tissue begin firing distress signals to the brainstem and spinal cord. The nervous system registers threat. It initiates a cascade of protective responses—muscle guarding, elevated sympathetic tone, altered pain-processing thresholds—that are designed to be temporary.
In a significant subset of patients, they are not temporary.
Section 2: The Nervous System Doesn’t Forget—Central Sensitization After Whiplash

Here is the concept that reframes everything about chronic whiplash: central sensitization.
Central sensitization is a state in which the central nervous system—the spinal cord and brain—becomes amplified in its response to sensory input. After a significant physical injury, particularly one involving rapid and involuntary loading of the spine, the nervous system can enter a state of heightened vigilance. Pain signals that would normally require a stronger stimulus to fire now trigger pain at much lower thresholds. Non-painful stimuli can become painful. The alarm system becomes hypersensitive—not broken, but recalibrated toward danger.
This is not psychological weakness. It is not a compensation claim. It is measurable, reproducible, and documented extensively in peer-reviewed literature.
A landmark study published in Pain (Banic et al., 2004) found that patients with chronic whiplash-associated disorders showed significantly lower pressure pain thresholds not only at the cervical spine—where the injury occurred—but also at remote sites: the forearm, the leg, the tibialis anterior. This widespread hypersensitivity is the fingerprint of central sensitization, not localized tissue damage. The nervous system has turned up the gain on pain throughout the entire body.
Several mechanisms drive this process. Persistent nociceptive input from injured soft tissues in the early weeks after injury can bombard the dorsal horn of the spinal cord, triggering wind-up: a process by which spinal cord neurons become increasingly responsive to repeated stimulation. Over time, this can produce long-term potentiation—essentially, the nervous system learns to be in pain. The synaptic connections that carry pain signals become structurally strengthened, even after the original tissue injury has healed.
Simultaneously, descending inhibitory pathways—the brain’s natural pain-suppression systems, which rely on serotonin, norepinephrine, and endogenous opioids—can become dysregulated. The brake on the pain system weakens at precisely the same time the accelerator strengthens.
This is why some patients with chronic whiplash report diffuse symptoms that seem disproportionate to their injury: widespread tenderness, sensitivity to light and sound, cognitive fog, fatigue, disturbed sleep, and emotional dysregulation. These are not separate complaints. They are expressions of a sensitized nervous system that has encoded the memory of the crash into its operating parameters.
The body is an archive. And this archive is not metaphorical.
“The nervous system learns to be in pain. The synaptic connections that carry pain signals become structurally strengthened, even after the original tissue injury has healed.”
Section 3: Who Develops Chronic Symptoms—What the Research Tells Us

Not every whiplash patient develops central sensitization. Understanding the predictors is not about assigning blame; it is about enabling early, targeted intervention before the sensitization cascade becomes entrenched.
The most comprehensive prospective research on whiplash outcomes has emerged from longitudinal cohort studies and the ongoing follow-up work building on the Quebec Task Force. Several consistent risk factors have been identified.
High initial pain intensity is the strongest single predictor of poor recovery. Patients who report severe neck pain in the first 24 to 48 hours after injury are significantly more likely to develop chronic whiplash-associated disorders than those with mild initial pain. This reflects the magnitude of early nociceptive input driving the sensitization process.
Cold hyperalgesia—abnormal sensitivity to cold stimuli applied to the skin—detected in the early post-injury period has emerged as a particularly robust early marker. A study by Sterling et al. (2003) in Pain found that patients who demonstrated cold hyperalgesia at baseline assessment were significantly more likely to have persistent symptoms at six months. This marker, measurable with straightforward bedside testing, captures early central sensitization before it becomes fully established—opening a window for intervention.
Fear-avoidance beliefs interact with—but do not independently cause—the neurobiological process. The expectation that movement will worsen injury leads to activity avoidance. Reduced movement reduces the sensorimotor input the nervous system needs to recalibrate. This avoidance, combined with heightened anxiety and pain catastrophizing, amplifies descending facilitation of pain signals and increases sympathetic activation. The psychology and the neurobiology are not two separate problems; they are a single feedback loop.
Pre-existing cervical degeneration matters, though not in the way insurance adjusters typically frame it. Degenerative changes in the cervical spine—reduced disc height, osteophytes, foraminal narrowing—reduce the spine’s capacity to absorb and dissipate collision forces. A previously asymptomatic degree of spondylosis can become clinically significant when paired with whiplash kinematics. The pre-existing condition amplified the injury. It does not diminish the legitimacy of the patient’s current suffering.
The collective message from this research is clear: the trajectory of whiplash recovery is not a simple function of how hard the impact was. It is a dynamic interaction between tissue injury, nervous system response, psychological state, and the quality and timing of clinical intervention. Early and appropriate treatment can interrupt the sensitization cascade. Delayed or purely passive treatment allows it to consolidate.
Section 4: The Spine as Memory—Altered Motor Control That Outlasts the Injury
Even in patients who do not develop overt central sensitization, whiplash injury leaves a legacy in the motor architecture of the cervical spine that standard follow-up protocols rarely assess.
The deep cervical flexors—the longus colli and longus capitis—are among the most critical stabilizers of the cervical spine. They maintain segmental alignment during movement and provide the foundational control that prevents excessive shear across vertebral discs and facet joint surfaces. Electromyographic studies by Jull and colleagues have consistently demonstrated that whiplash injury disrupts the recruitment patterns of these deep stabilizers. Patients with chronic whiplash show delayed activation and significantly reduced endurance of the deep cervical flexors compared with asymptomatic controls—not just in the acute phase, but months and years after the original injury.
In their place, the more superficial cervical muscles—the sternocleidomastoid and the anterior scalenes—tend to compensate. But these muscles are poorly suited to segmental stabilization. They cross multiple spinal levels, generate substantial compressive load, and fatigue quickly. Their chronic overactivation is a major driver of the persistent headaches, upper trapezius tension, arm paresthesias, and jaw symptoms that many whiplash patients carry long after their initial presentation.
The spine has reorganized itself around the injury. It has found a way to function, but the architecture of that function is compromised. Every movement, every hour of desk work, every load placed on the cervical spine is being managed by a system that is compensating rather than coordinating efficiently.
This altered motor control pattern is not merely a biomechanical inconvenience. It is an ongoing source of nociceptive input. Facet joint capsules stressed by abnormal segmental kinematics continue to generate pain signals. Muscle spindles in chronically shortened or overactivated muscles provide distorted proprioceptive feedback that the nervous system must constantly process and reconcile.
Research by Treleaven and colleagues has documented impaired cervical joint position sense in chronic whiplash patients—a measurable deficit in the ability to accurately perceive where one’s head is in space after a movement. This proprioceptive impairment contributes directly to the dizziness, unsteadiness, and visual disturbances that many whiplash patients report, and that are frequently dismissed without adequate investigation.
The spine has a memory. Not a cognitive memory—the patient may barely recall the accident with any emotional charge by now. But a motor memory. A proprioceptive memory. A structural memory carried in every movement pattern, every postural adaptation, every millisecond of altered feedback flowing upward to the central nervous system.
“The spine has a motor memory, a proprioceptive memory, a structural memory—carried in every movement pattern and every millisecond of altered feedback flowing upward to the central nervous system.”
Section 5: Rewriting the Archive—What Effective Whiplash Rehabilitation Actually Requires

If the problem is not simply damaged tissue but an altered nervous system and a reorganized motor control system, then treatment that addresses only tissue—rest, anti-inflammatories, passive modalities—is necessarily incomplete. It treats the symptom without addressing the mechanism.
Effective rehabilitation for chronic and sub-acute whiplash must work simultaneously across three domains: the mechanical, the neurological, and the psychological. These are not optional additions to a treatment plan. They are integral to interrupting the feedback loops that sustain the chronic pain state.
Restoring deep cervical flexor function is the mechanical foundation. Exercises targeting the longus colli and longus capitis—performed with precision at low loads, with real-time feedback to prevent compensatory superficial muscle recruitment—gradually rebuild the normal architecture of cervical stability. Jull’s cranio-cervical flexion test provides a reliable clinical benchmark for tracking this progress. The evidence base supporting deep cervical flexor training for whiplash outcomes is among the most consistent in musculoskeletal rehabilitation research.
Sensorimotor rehabilitation addresses the proprioceptive deficits and altered pain-processing that characterize central sensitization. Gaze stabilization exercises, head-repositioning accuracy training, and progressive, graded exposure to pain-free cervical range of motion all contribute to recalibrating the nervous system’s map of the body in space. The goal is not simply to lengthen a tight muscle. The goal is to teach the nervous system what safe movement feels like again—to give it new data that overrides the threat-encoded patterns of the post-injury period.
Pain neuroscience education—helping patients understand the biology of what is happening in their nervous system—has been shown in randomized controlled trials to reduce pain catastrophizing, improve physical performance, and decrease disability in chronic pain populations. When patients understand that their pain is being maintained by a sensitized nervous system rather than active, ongoing tissue damage, the fear that drives avoidance begins to dissolve. And fear-avoidance, as we have established, is one of the key perpetuating factors in the chronic whiplash cycle.
Manual therapy directed at the cervical and upper thoracic spine reduces nociceptive input by restoring segmental mobility, decreasing facet joint mechanical loading, and engaging descending inhibitory pathways through a neurological mechanism. Spinal manipulation and mobilization produce measurable effects on systemic pain thresholds—a finding that reflects their neurological reach, not merely their mechanical effect.
Timing matters profoundly. Early intervention—beginning within the first weeks after injury—can interrupt the sensitization process before it consolidates. The neuroplasticity that makes early rehabilitation effective also means that delay allows maladaptive patterns to become structural. The window is real, and it closes gradually.
I tell every patient the same thing: the weeks immediately after a collision are not the time to wait and see. They are the time to act. Not from fear—fear only reinforces the sensitized state. From understanding. The archive is being written in real time. What happens in these early months determines what that archive contains.
The neuroplasticity that makes early rehabilitation effective also means that delay allows maladaptive patterns to consolidate. Early intervention—within the first weeks after injury—can interrupt the sensitization cascade before it becomes structural. The window is real, and it narrows over time.
Section 6: Why the Medical System Keeps Getting This Wrong
The dominant framework for whiplash in emergency medicine, insurance systems, and much of primary care remains a structural, tissue-damage model. Imaging reveals no significant injury; therefore, the patient should recover within six to twelve weeks. If symptoms persist beyond that window, the explanation offered is often psychological—secondary gain, anxiety, compensation-seeking behavior.
This framework is not supported by the science. It is contradicted by it.
A systematic review by Holm et al. published in Spine found that symptom persistence at twelve months was significantly predicted by initial injury severity and early pain intensity—not by whether the patient had a litigation claim, not by pre-existing psychological factors as primary drivers. The biology is real. The suffering is real. And dismissing it as psychological does not make it less neurological; it simply ensures the patient receives inadequate treatment.
The core error is conflating two distinct things. Structural integrity—whether bones and discs appear intact on imaging—is not the same as functional integrity—whether the nervous system is processing pain signals appropriately, whether motor control patterns are properly coordinated, whether pain thresholds have been pathologically lowered. A patient can have a completely normal MRI and a profoundly disrupted nervous system. Both things are simultaneously true.
The consequences of this diagnostic blind spot are significant. Patients told early that their symptoms should resolve quickly experience confusion and self-doubt when they don’t. The gap between expected recovery and actual experience becomes its own source of distress, which—through the mechanisms we have now explored—further amplifies the sensitized pain system. The medical system, in its attempt to reassure, inadvertently invalidates.
What patients with significant whiplash injuries actually need is accurate information: that this injury can disrupt the nervous system in ways imaging cannot detect; that recovery is possible but requires specific, targeted, and sustained rehabilitation; that their experience is neurobiologically real; and that the timeline for meaningful recovery from significant whiplash is measured in months—not the two to four weeks that insurance adjusters and discharge summaries so frequently cite.
Conclusion: The Archive Can Be Rewritten
The thesis of this essay is not a metaphor. It is a neurobiological statement.
Long after the mind has moved on from the crash—filed it away, told the story at dinner, stopped replaying it at 2 a.m.—the body continues to operate under the protocols established in those 300 milliseconds of impact. The cervical musculature has reorganized around absent deep stability. The proprioceptive networks are sending distorted signals to a sensitized spinal cord. The pain system, amplified by weeks or months of nociceptive input, has lowered its threshold for alarm.
Bodies remember what minds forget. And unless that archive is read carefully—by clinicians trained to look beyond imaging, by patients given accurate information about their own neurobiology, by a healthcare system willing to update its model—those encoded memories persist as pain, restriction, fatigue, and diminished capacity for life.
The genuinely good news is that the nervous system is plastic. It changes in response to persistent threat. But it also changes in response to persistent safety, skilled rehabilitation, and accurate understanding. The motor control patterns that organized around injury can, with specific and sustained work, reorganize around health. The sensitized system can recalibrate. The archive can be rewritten.
This is the real work of whiplash rehabilitation. It is slow, it is unglamorous, and it demands more from both the clinician and the patient than passive treatment and wishful waiting. But it is grounded in the best science available, and it works.
The body remembers. But memory is not destiny. With the right guidance and the right treatment, the story the body tells can change.
“Memory is not destiny. With the right guidance and the right treatment, the story the body tells can change.”
