Definition and Epidemiology
Cervicogenic headache (CGH) is a secondary headache syndrome in which pain arises from the cervical spine (neck) and is perceived in the head or face. In practical terms, CGH typically presents as a unilateral headache that starts in the neck or occipital region and radiates to the frontotemporal or orbital areas. It is often associated with neck stiffness or restricted range of motion, and head pain can be triggered or worsened by neck movements, sustained awkward postures, or pressure on tender neck structures. CGH is classified by the International Headache Society (IHS) as a headache attributed to a cervical musculoskeletal disorder (a secondary headache), distinguishing it from primary headaches like migraine or tension-type headache.
In terms of epidemiology, true CGH is relatively uncommon compared to primary headaches. Population studies estimate that CGH accounts for around 0.4% to 4% of all headaches seen in clinics. Some clinical pain specialists report a higher proportion (up to 15–20%) of chronic recurrent headaches may have a cervicogenic origin, reflecting the referral patterns to specialty clinics. CGH can affect both sexes equally (female-to-male ratio ~1:1). It most commonly begins in adulthood (30s to 40s) and may be associated with a history of neck injury or degenerative changes, although many patients do not seek diagnosis until later in life . Given its often subtle presentation and overlap with other headaches, CGH is frequently underdiagnosed or misdiagnosed as a primary headache, underscoring the importance of clinician awareness of this entity.
Pathophysiology and the Trigeminocervical Connection
CGH arises from nociceptive structures in the neck, particularly those innervated by the upper three cervical spinal nerves (C1, C2, C3). Pain-sensitive cervical structures include the upper cervical zygapophyseal (facet) joints, atlanto-occipital and atlanto-axial joints, intervertebral discs, cervical muscles and ligaments, and cervical nerve roots themselves. Irritation or injury of these structures (for example, due to arthritis, disk pathology, trauma like whiplash, or muscle spasm) can trigger pain signals that are perceived as headache. The key anatomical substrate for this referral of pain is the trigeminocervical nucleus (TCN), sometimes called the trigeminocervical complex. This is a region in the upper cervical spinal cord (the C1–C3 dorsal horn) contiguous with the descending spinal tract of the trigeminal nerve .

Within the trigeminocervical nucleus, afferent input from the upper cervical nerves converges with input from the trigeminal nerve, which supplies the face and head . Because of this convergence, the brain can interpret pain from the neck as originating in the head – a phenomenon explaining why CGH pain often radiates from the occipital region to the temple or eye. This same pathway also means that primary headaches (like migraine) can cause referred pain in the neck. Indeed, experimental studies show a bidirectional facilitation: stimulating the upper cervical (greater occipital) nerve can increase excitability of trigeminal pain pathways, and stimulating trigeminal structures (like the dura) can sensitize cervical neurons. This neuroanatomical overlap accounts for the symptom overlap between CGH and migraines and underscores that a shared trigemino-cervical pathway is involved in head-neck pain syndromes.
Beyond the convergence mechanism, chronic nociceptive input from the neck can induce central sensitization in the trigeminocervical nucleus. Over time, this can lower pain thresholds and lead to heightened sensitivity (hyperalgesia or allodynia) in the head and neck. For example, neck trauma or longstanding cervical dysfunction may cause the Trigeminocervical nucleus (TCN) neurons to become hyperexcitable, analogous to what occurs in chronic migraine. This can result in pericranial muscle tenderness and the spread of pain beyond the original neck source. In some patients, prolonged nociceptive barrage leads to a cycle of pain and muscle spasm, and even activation of cranial autonomic pathways (via connections of the TCN to brainstem autonomic centers) that can occasionally produce symptoms like nausea or blurred vision that mimic primary headaches. However, these features are usually milder in CGH than in migraine. Notably, the C2-3 zygapophyseal joint (innervated by the C3 dorsal ramus via the third occipital nerve) is implicated as the most common source of CGH; studies suggest up to ~70% of cervicogenic headaches originate from arthropathy or dysfunction at C2-3 . Other contributors include C1-2 (atlanto-axial) joint pathology, C2-3 disc lesions, or upper cervical muscle trigger points. Identifying the precise pathological source in CGH can be challenging, but it is often narrowed down by diagnostic blocks (see below) and detailed examination.
Clinical Features and Diagnostic Criteria

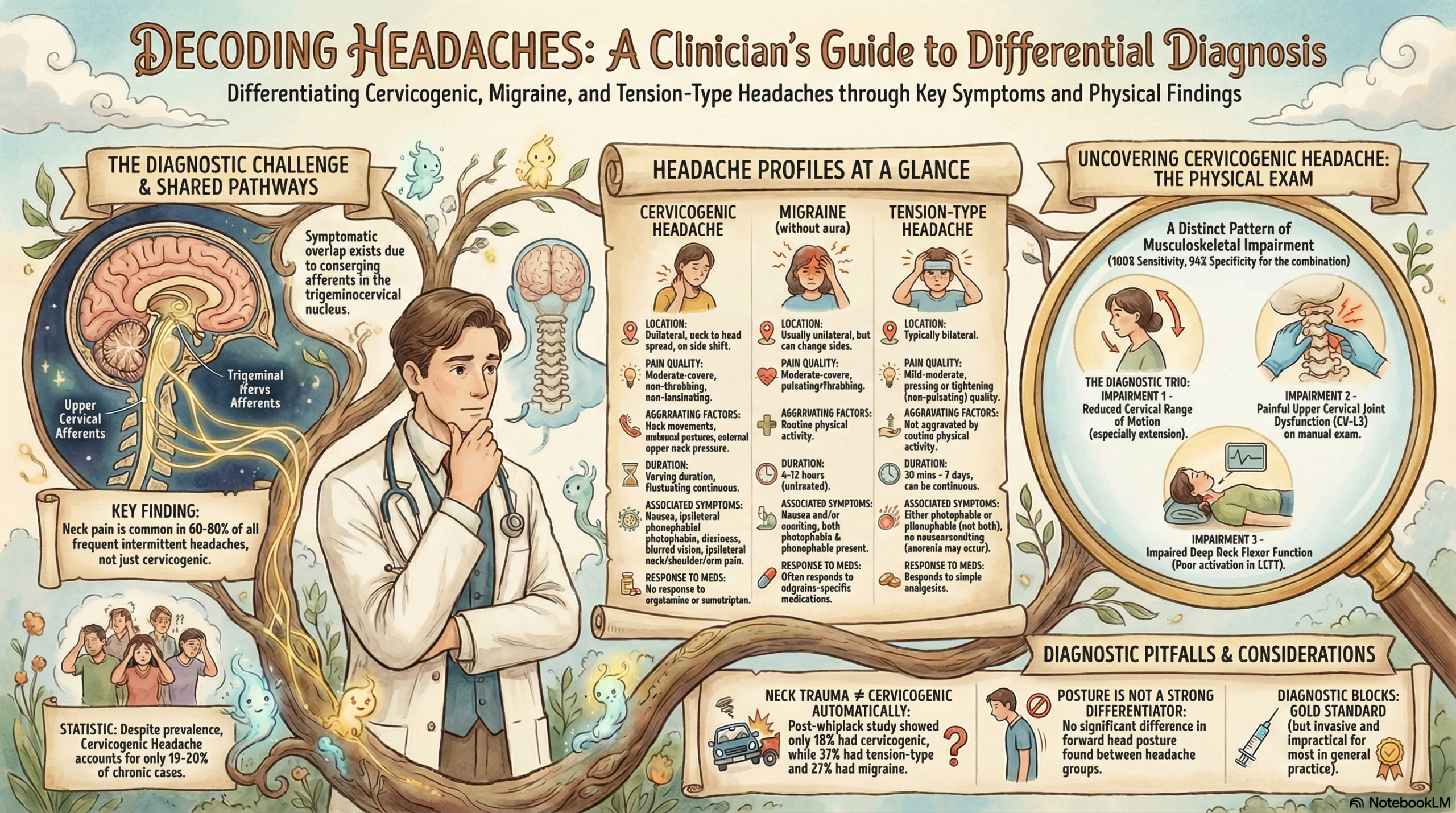
Clinically, cervicogenic headache typically presents as a unilateral pain that starts in the neck or suboccipital area and spreads to the ipsilateral head (occipital, temporal, or frontal regions) . The pain is often described as a dull, aching pressure rather than a pulsating or throbbing pain; it is usually moderate in intensity but can fluctuate in severity. Unlike migraine, CGH pain tends not to be lancinating or sharp (those descriptors are more suggestive of neuralgias). A hallmark feature is the association with neck movements or positions: the headache is precipitated or worsened by certain neck motions (e.g. rotation, extension) or by sustained awkward postures (such as prolonged desk work). Patients often report restricted cervical range of motion and may have neck stiffness. On examination, there is frequently ipsilateral neck tenderness, especially over upper cervical joints or musculature, and reproduction of the headache with pressure on these structures (e.g. pressing over the C2-3 facet joint or suboccipital muscle insertions may trigger the familiar head pain) . Associated symptoms can include ipsilateral neck/shoulder pain or arm discomfort, since the cervical nerves also supply those regions. Unlike migraines, severe nausea, vomiting, photophobia or phonophobia are typically absent or only mild in CGH – some patients have light or sound sensitivity, but these are less pronounced than in migraine and may relate to co-existing tension in neck muscles. Similarly, CGH is not usually accompanied by neurologic aura. These distinctions, however, are not absolute, so clinicians must use a combination of history, exam, and diagnostic studies to make the diagnosis.
Formal diagnostic criteria for CGH have been established by the International Classification of Headache Disorders, 3rd edition (ICHD-3). In summary, the ICHD-3 defines CGH as a headache caused by a cervical spine disorder, with the following key features:
In practice, criterion C(4) – the abolition of headache with a diagnostic anesthetic block in the neck – is considered the gold-standard confirmation of CGH. For example, a complete relief of the headache after anesthetizing the C2-3 facet joint or the greater occipital nerve strongly implicates that structure in the pain generation. However, performing diagnostic blocks is invasive; thus, many clinicians make a presumptive CGH diagnosis based on history and exam findings consistent with neck-origin pain, after excluding other causes.
Several clinical classification schemes have also been proposed. The Cervicogenic Headache International Study Group (CHISG) emphasizes practical clinical criteria, such as a unilateral headache with consistent side-lock (the pain does not switch sides between episodes), pain provoked by neck movement or sustained posture, and neck tenderness or restricted motion on exam . An important point is that CGH is typically unremittingly one-sided (always on the same side), whereas migraines can alternate sides between attacks. CGH pain may be episodic or chronic continuous, and its duration can vary widely (from hours to days, or a low-grade continuous neck ache punctuated by severe flares). Relief of the headache with nerve blocks or resolution of the presumed neck pathology (e.g. successful treatment of a cervical disc herniation) is considered supportive evidence of the diagnosis. Advanced imaging (MRI or CT of the cervical spine) is often performed to rule out serious structural lesions, but it has limited utility in definitively diagnosing CGH – degenerative changes are common in asymptomatic individuals, and mild disc or joint abnormalities on MRI do not prove causation. Thus, the diagnosis of CGH is primarily clinical, assisted by blocks when needed, and requires careful exclusion of other headache disorders.
Differential Diagnosis
A structured differential diagnosis is critical, as CGH can be confused with, or even coexist with, several other headache types. Key considerations in the differential include primary headaches (migraine and tension-type being the most common) and occipital neuralgia, as well as other causes of unilateral head pain. Below, we contrast CGH with some of these entities:
In summary, CGH can be distinguished from primary headaches by its neck-origin characteristics: a fixed unilateral pain linked to neck movement or tender cervical structures, often accompanied by neck stiffness and relief with targeted blocks. Table 1 below summarizes some key differentiating features:
- Cervicogenic Headache: Unilateral (side-locked) neck/occipital pain referring to frontotemporal regions; dull aching quality; provoked by neck movement or pressure; often reduced neck ROM and neck tenderness; mild or no nausea/photophobia; no aura; improves with cervical blocks .
- Migraine: Unilateral (but can alternate sides) throbbing pain usually starting in frontotemporal region; often severe; triggered by stress, hormones, etc. (not specifically neck motion); associated with nausea, vomiting, photophobia/phonophobia; may have aura; physical activity aggravates; responds to migraine medications (e.g. triptans) .
- Tension-Type Headache: Bilateral, band-like pressure or tightness; mild to moderate intensity; not activity-dependent; no significant nausea or aura; may have pericranial muscle tenderness but not true neck movement-provoked pain; generally responsive to analgesics and stress management .
- Occipital Neuralgia: Paroxysmal stabbing or shock-like pains in occipital region; unilateral (sometimes bilateral) but follows nerve distribution; pain is brief but can recur; tenderness over occipital nerve; triggers include neck pressure or occipital nerve compression; often responds to occipital nerve block; no significant photophobia or nausea, but pain can be very intense during jabs .
Recognizing these differences is crucial for appropriate management, as treatments effective for migraine or tension headache (for example, triptans or high-dose NSAIDs) usually do not adequately relieve a true cervicogenic headache. Conversely, treatments that address cervical pathology (like chiropractic) would not benefit a primary migraine. In unclear cases, diagnostic anesthetic blocks of cervical structures can help confirm CGH versus a primary headache disorder.
Treatment and Management Strategies
Managing cervicogenic headache often requires a multifaceted approach, targeting the underlying cervical pathology and the resultant pain. Treatments can be broadly divided into conservative (non-invasive), pharmacologic, and interventional strategies. Evidence-based guidelines emphasize starting with conservative therapies, and reserving more invasive interventions for refractory cases. It is important to set expectations with patients that CGH treatment is usually aimed at control rather than permanent cure – the condition tends to be chronic-recurrent, though effective management can greatly improve quality of life.
Conservative Therapies: Manual Therapy and Exercise
Chiropractic therapy and manual manipulation are considered first-line treatments for CGH. The rationale is that many CGH cases stem from joint dysfunction or muscular imbalance in the upper cervical region; thus, improving cervical mobility, posture, and muscle function can reduce the nociceptive drive. Skilled manual therapy techniques – including spinal mobilization or high-velocity low-amplitude manipulation of the cervical and thoracic spine, soft tissue massage, and trigger point release – aim to restore normal movement in the facet joints and alleviate muscle tension. These techniques may directly reduce pain by relieving joint stress and may also modulate pain through neurophysiological mechanisms (stimulation of mechanoreceptors, gating of pain signals in the spinal cord). Exercise therapy complements manual treatments by strengthening and retraining the cervical and scapular musculature. A common focus is on deep neck flexor strengthening, scapulothoracic posture correction, and stretching of tight suboccipital and chest muscles, thereby addressing forward-head posture or other biomechanical contributors to CGH.
Evidence supports the effectiveness of combining manual and exercise therapy. In a notable randomized trial by Jull et al., patients with CGH were treated with manipulative therapy to the cervical spine plus a low-load endurance exercise program for the neck and shoulder muscles. After 12 months, about 72% of treated patients had significant reductions in headache frequency and intensity, compared to controls. Many achieved prolonged relief, demonstrating that the benefits persisted long-term. A 2022 systematic review and meta-analysis (Bini et al.) that pooled data from 20 studies found moderate-quality evidence that manual therapy and exercises lead to clinically meaningful reductions in CGH headache frequency, intensity, and disability, both in the short term and sustained over months. Spinal manipulation, in particular, showed positive outcomes in high-quality trials, although results can vary and a combination approach is often recommended. The general protocol is to undergo 8–12 sessions of physiotherapy-based treatment over 6–8 weeks. Patients are taught home exercises to maintain improvements. It’s important to note that symptoms might transiently worsen at the start of therapy due to mobilizing painful structures, but this usually improves as strength and mobility increase. Overall, conservative management focusing on cervical rehabilitation is effective for a substantial subset of patients and carries a low risk of adverse effects. Beyond physical techniques, patient education (ergonomic advice, proper posture, avoiding sustained head-forward positions) and behavioral therapy (like biofeedback or cognitive-behavioral therapy for pain coping) can provide additional benefit in chronic cases.
Pharmacologic Treatments
Medications play a supportive role in CGH management, primarily for symptom relief. Unlike migraines or cluster headaches, there is no specific “abortive” medication uniquely effective for cervicogenic headache; however, various analgesics and adjuvant pain modulators are used based on clinical judgment:
- Analgesics: Simple analgesics such as acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly tried for acute CGH pain. NSAIDs may help if there is an inflammatory component (e.g. facet joint arthritis or muscle strain). In practice, these medications often provide only partial relief in CGH, and some patients get little benefit . Nonetheless, they are reasonable first-line agents for mild to moderate headaches given their availability and familiarity. Caffeine-containing combination analgesics (e.g. aspirin/acetaminophen/caffeine) have also been used, as caffeine may enhance analgesic effect (similar to tension-type headache treatment) and some patients report relief with these . Caution is warranted to avoid medication overuse; frequent use of analgesics can lead to rebound headaches.
- Muscle Relaxants: If there is significant neck muscle spasm, short-term use of muscle relaxants (such as tizanidine or cyclobenzaprine at night) can be helpful to break the cycle of pain and tightness. Muscle relaxants may improve cervical range of motion and reduce referred muscle tension headache components. These are used as needed; sedating effects often limit daytime use.
- Neuropathic Pain Modulators: Given the chronic nature of CGH and the central sensitization component, preventive medications similar to those for chronic migraine or neuropathic pain are sometimes employed. Tricyclic antidepressants (e.g. amitriptyline or nortriptyline) or SNRIs (e.g. venlafaxine, duloxetine) can be used at low doses to help modulate pain pathways and improve sleep . Likewise, certain anticonvulsants such as gabapentin or topiramate have been tried in CGH to reduce neuronal hyperexcitability . While these uses are off-label and specific evidence in CGH is limited, clinicians may extrapolate from their efficacy in other chronic headache disorders. For example, topiramate is effective in migraine prevention, and gabapentin can reduce neuropathic pain; some patients with CGH have reported reduced headache frequency on these agents, particularly if neck injury has led to nerve irritation.
- Other Medications: There is little evidence that CGH responds to migraine-specific drugs like triptans or ergot derivatives. Studies indicate that triptans, which target the trigeminovascular inflammation in migraine, generally do not alleviate cervicogenic headaches . This lack of effect can actually be a clue that the headache is cervicogenic rather than migrainous. Indomethacin, which is famously effective in indomethacin-sensitive headaches like hemicrania continua or paroxysmal hemicrania, usually has no effect on CGH – again highlighting a different mechanism. Some practitioners have explored botulinum toxin type A injections for CGH, especially in cases with significant neck muscle involvement. Botulinum toxin A (onabotulinumtoxinA) is well-established for chronic migraine prevention, and while CGH is not the same mechanism, a few case reports and small series have suggested potential benefit in reducing CGH frequency/severity in some patients . The toxin is thought to help by reducing muscle spasm and possibly downregulating pain transmitters at the nerve endings. However, evidence for botulinum toxin in CGH is not yet robust; a recent systematic review in veterans with chronic headaches found it effective for chronic migraine, but efficacy in tension-type or cervicogenic headache was not clearly supported . Thus, botulinum toxin is not a first-line treatment for CGH, though it might be considered in refractory cases with muscle-dominant pain.
In summary, pharmacotherapy for CGH is generally multimodal and borrowed from general pain management principles. Medications such as NSAIDs, acetaminophen, or muscle relaxers address the musculoskeletal aspect, while tricyclics or gabapentinoids can target the centralized pain component. It is important to manage expectations – these drugs often do not completely eliminate the headaches, but they can reduce pain levels and improve function when used appropriately. Always ensure the patient is not simply treating symptoms without addressing the cause; drugs should be seen as adjuncts to the primary mechanical treatments (physiotherapy or interventions). Over-reliance on analgesics should be avoided to prevent rebound headaches.
Interventional Treatments
For patients with severe or persistent cervicogenic headaches that do not respond sufficiently to conservative measures, interventional procedures can offer significant relief. These treatments target the pain generators or neural pathways in the cervical region. The choice of intervention often depends on identifying which cervical structure is at fault (e.g. a particular facet joint vs. the occipital nerve). Common interventional options include:
- Nerve Blocks: Local anesthetic blocks can be used diagnostically and therapeutically. A greater occipital nerve (GON) block is a simple clinic procedure where anesthetic (often with steroid) is injected near the emergence of the C2 dorsal ramus (just below the superior nuchal line). GON blocks can relieve CGH pain in many cases, at least transiently, especially if the headache involves the occipital region . This block essentially numbs the C2 distribution and can break the headache cycle; relief supports the diagnosis and can last days to weeks. Similarly, lesser occipital nerve blocks (C2/C3) can be done if pain extends laterally. For CGH stemming from facet joints, medial branch blocks of the C2-3 facet (third occipital nerve) or C1-2 facet (C2 nerve) can pinpoint the source. If a patient gets >90% pain relief from a properly performed diagnostic block of a facet joint nerve, it strongly suggests that joint is the pain generator . Clinically, a series of anesthetic/steroid blocks may also provide medium-term relief by reducing inflammation in the facet joints or around nerve roots. Epidural steroid injections at the cervical level are another option, especially if a cervical disc herniation or spondylosis is contributing to nerve irritation. There is some evidence that cervical epidural steroid injections can reduce CGH pain by alleviating nerve root inflammation and breaking the pain cycle . These injections are typically done under fluoroscopy for safety.
- Radiofrequency Ablation (RFA): If a patient has confirmed relief from a facet joint nerve block but pain recurs, radiofrequency neurotomy can be performed to lesion the nerve and provide longer-lasting relief. In CGH, the most common target is the third occipital nerve, which innervates the C2-3 facet joint (often implicated in CGH). RFA of the third occipital nerve after positive blocks has been shown to significantly reduce headache frequency and intensity in a majority of patients, with relief lasting on the order of 6–12 months or more in successful cases . Technique is important; earlier studies showed variable results, but improved methods (e.g. using multiple lesion sites to account for nerve variability) achieved up to 88% complete relief in one series . RFA can also be applied to the C2 dorsal root ganglion or lateral C1-2 joint innervation if those are identified sources. Essentially, RFA “burns” the small pain-transmitting nerve fibers, preventing them from carrying pain signals. This is minimally invasive (done with needles under X-ray guidance) and can be repeated if nerves regenerate. Patients should be counseled that numbness or loss of sensation in a small patch of skin can occur, and in rare cases, symptoms like occipital numbness or neuroma formation can happen, but overall RFA is considered a safe and effective intervention in experienced hands.
- Atlanto-axial or Atlanto-occipital Joint Injections: Less commonly, if the C1-2 (atlanto-axial) joint or C0-1 (atlanto-occipital) joint is suspected as the pain source (e.g. pain provoked by head rotation suggests C1-2 involvement , or pain with head nodding for C0-1), targeted injections can be performed into these upper cervical joints. Distension of the lateral C1-2 joint in volunteers reproduces occipital headache, supporting it as a cause in some patients . Intra-articular corticosteroid injections in the lateral atlanto-axial joint have shown short-term efficacy in reducing CGH in uncontrolled reports . Due to the proximity of the vertebral artery and spinal cord, these injections must be done very carefully (often with CT or fluoroscopic guidance) . If successful, they can reduce inflammation in an arthritic joint and provide relief for weeks to months. If pain recurs and is clearly from these joints, some patients may undergo RFA of the C1-2 joint innervation or even surgical fusion (arthrodesis) of C1-2 in extreme cases . Atlanto-occipital joint involvement is rarer; conservative therapy is usually preferred, and injections are less commonly done there (due to even tighter safety margins).
- Other Interventions: In recalcitrant cases, additional procedures have been explored. Cryoneurolysis(cryoablation) of the C2 or C3 nerves is an alternative to RFA – it involves freezing the nerve to inactivate it, and can provide a few months of relief if RFA is not available. Peripheral nerve stimulation of the occipital nerves (implanting a small electrode that delivers electrical stimulation to modulate pain) has been tried in chronic occipital headache conditions and might help some CGH patients, although evidence is preliminary. Sphenopalatine ganglion block or cervical sympathetic block (stellate ganglion block) have been mentioned in some case series for cervicogenic headaches, especially if there are autonomic features or if a sympathetic-maintained pain component is suspected . Transcutaneous electrical nerve stimulation (TENS) is a non-invasive modality that some physical therapy programs use; a small randomized trial suggested TENS to the upper cervical region can reduce CGH pain, presumably by closing the “pain gate” at the spinal cord level . While not a definitive treatment, it can be a helpful adjunct with virtually no risk.
- Surgical Options: Surgery is rarely needed for CGH unless a definitive surgically correctable lesion is identified (for example, a benign tumor compressing the upper cervical nerves, or severe atlanto-axial instability from trauma or rheumatoid arthritis). One historical surgical approach for severe CGH has been C2 dorsal root ganglion decompression or even C1-C3 rhizotomy (cutting the nerves) in extreme cases . Posterior fossa decompression would be indicated if a Chiari malformation is the culprit. In select cases of proven C2-3 discogenic headache (a rare scenario), an anterior cervical discectomy and fusion at C2-3 reportedly relieved headaches . These invasive procedures are last resorts and should only be considered when all conservative and minimally invasive measures have failed and the patient’s functioning is severely impaired by the headaches.
When choosing interventional treatments, it is often wise to proceed in a stepwise fashion: use diagnostic blocks to confirm the suspected pain generator, then apply a more definitive treatment like RFA or surgical fixation if appropriate. For example, if a patient’s headache is completely relieved for the duration of a local anesthetic block of the third occipital nerve, one could then proceed to third occipital nerve RFA for longer relief . If an epidural injection yields significant temporary relief in a patient with a C6-7 disk protrusion and CGH features, it suggests a nerve root inflammatory component that might warrant neurosurgical evaluation or repeat injections. It’s also common to combine therapies – for instance, doing nerve blocks to facilitate participation in a rehab exercise program, or using medication to manage pain flares while awaiting an intervention.
The evidence base for interventional treatments in CGH varies. A landmark review by Bogduk & Govind (2009) found strong evidence supporting the use of cervical medial branch blocks and RFA for CGH after positive blocks, while evidence for many other interventions was limited  . Since then, additional studies have reinforced that interventions like third occipital nerve RFA can be highly effective in well-selected patients, often producing significant improvement in headache-related disability. However, these are not usually permanent cures – nerves can regenerate, and some patients need repeat procedures after 6–18 months. Occipital nerve blocks are low-risk and can be repeated periodically if they help; some patients use them as needed for flares. Importantly, none of these interventions should be seen as standalone cures; they are part of a comprehensive management plan. For instance, after an RFA or block, patients should continue cervical exercises to maintain motion and possibly lengthen the pain-free interval .
Finally, it is crucial to address patient expectations and psychosocial factors in chronic CGH. Since CGH often requires ongoing management rather than one-time cure, patients may become frustrated or anxious. Multidisciplinary care – involving primary care, neurologists, pain specialists, physical therapists, and occasionally psychologists for pain coping – yields the best outcomes . Educating patients that CGH is a real, physiological pain (due to nerve convergence) and not “in their head” can validate their experience and improve compliance with therapy. With an individualized combination of therapies, most patients with cervicogenic headache can achieve substantial relief and improved function. The goal is to accurately diagnose the condition (distinguishing it from mimics), treat any reversible cervical pathology, reduce the frequency and severity of headaches, and ultimately improve the patient’s quality of life.
References: Cervicogenic headache is an area of active research, and readers are encouraged to consult recent systematic reviews and guidelines for up-to-date evidence on management. Key references include the International Headache Society’s ICHD-3 classification for diagnostic criteria , the systematic review by Bini et al. 2022 on manual therapy efficacy , and expert analyses of invasive treatments , among others. By integrating clinical insight with evidence-based interventions, clinicians can greatly improve diagnostic accuracy and treatment outcomes for patients suffering from cervicogenic headaches.
