Embracing Probability: Why Medicine Can’t Promise Certainty, and Why That’s Not a Failure
The question comes at the end of almost every initial consultation. The patient has been through the intake, the examination, the explanation of findings. They’ve nodded through the conversation about soft tissue mechanics and healing timelines and the gap between what the imaging shows and what the body actually feels. And then, as they’re pulling on their jacket, they turn around and ask it:
“So I’m going to be okay, right?”
They want a yes. They want certainty. They want someone in a white coat to tell them that what happened is over, that the body has a script it will follow, and that it ends with them feeling exactly the way they did before the rear-end collision at the intersection on a Tuesday afternoon.
I understand the desire. When your body has betrayed you — when a moment of violence you didn’t choose has left you with pain you didn’t ask for — what you want most is solid ground. You want someone to tell you the future.
And here is the honest answer, the one that good medicine has to give: I can tell you about probabilities. I cannot tell you about certainties. And the difference between those two things is not a failure of science. It’s the beginning of it.
This essay is about probability — specifically, about what the research tells us regarding the recurrence of low back pain after a collision, why the probabilistic nature of that risk matters for how patients are treated and followed, and why the willingness to embrace uncertainty rather than paper over it is what separates rigorous clinical practice from reassuring fiction.
The Silence Before the Accident — Understanding Baseline Risk
To understand why prior low back pain matters so much to recurrence after a collision, we first need to understand how common low back pain is in the general population — and how often it goes into remission without fully resolving.
Low back pain is the leading cause of disability worldwide. Point prevalence estimates suggest that approximately 12% of the global adult population is experiencing low back pain at any given moment. Lifetime prevalence is substantially higher — estimates range from 60% to 85% depending on the population studied. Most episodes resolve within four to six weeks, which has historically led clinicians to characterize low back pain as a self-limiting condition.
But “resolved” is not the same as “gone.”
A landmark 2006 systematic review examining the natural history of low back pain found that within one year of a first episode, recurrence rates ranged from 24% to 80% depending on the population and the definition of recurrence used. A 2019 meta-analysis published in The Lancet found that among patients who had “recovered” from an acute episode of low back pain, one in three reported a recurrence within a year, and a substantial proportion had residual pain that never fully resolved despite their self-reported recovery.
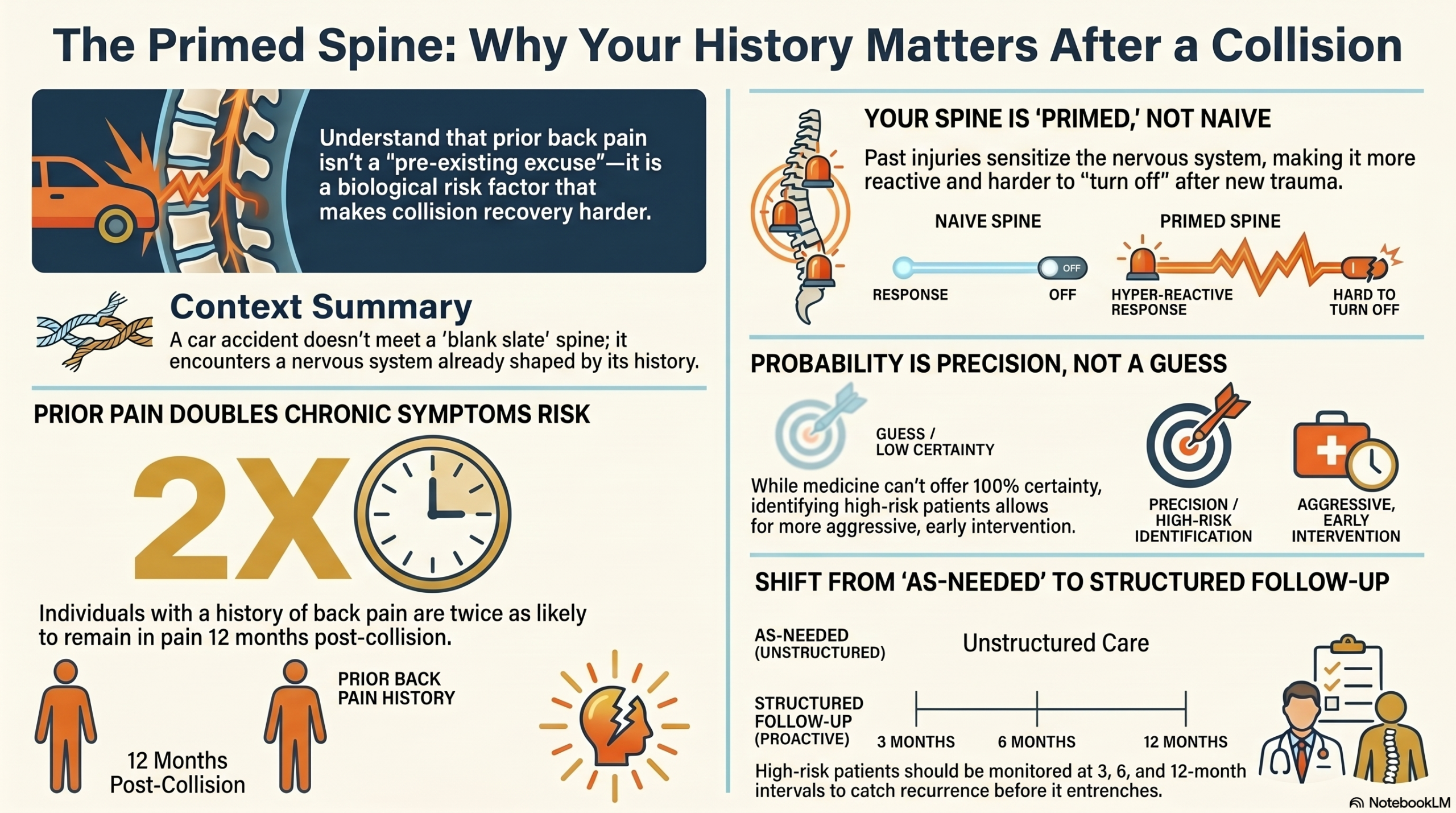
What does this mean in practice? It means a significant proportion of people who walk into a motor vehicle collision clinic having had no back pain for months — or even years — are carrying a spinal system that has already been sensitized, already been through inflammatory cycles, already accumulated some degree of structural change, and has a documented propensity to become symptomatic again when stressed.
“The collision is not encountering a naive spine. It is encountering a history.”
The Evidence on Prior Low Back Pain and Collision-Related Recurrence
Multiple prospective cohort studies have examined what predicts who develops chronic low back pain after a motor vehicle collision. Across the literature, prior history of low back pain is one of the most consistently identified predictors of poor outcome.
Why does prior history carry this predictive weight? The answer is neurobiological. An individual who has had a prior episode of low back pain has already activated the central sensitization process. Their dorsal horn neurons have already been potentiated. Their descending inhibitory pathways have already been challenged. Their pain-processing system has been recalibrated to be more vigilant about threat signals from the lumbar spine.
When a collision then delivers acute nociceptive input into this already-primed system, the sensitization is easier to re-establish — and harder to extinguish. The tissue heals, but the nervous system remains on alert.

What Probability Actually Means in Clinical Medicine
At this point, a sophisticated reader might object: isn’t this all just correlation? Doesn’t it simply mean that people with prior pain are more likely to be pain-prone by temperament? Maybe the collision isn’t actually doing anything different — maybe we’re just seeing a vulnerable population express its vulnerability.
This objection is worth taking seriously, because it reflects a genuine methodological challenge in longitudinal pain research. But the evidence doesn’t support the pure vulnerability interpretation.
Here’s why. If prior pain history were simply selecting for pain-prone individuals who would have gotten worse regardless of the collision, we would expect those individuals to be on a continuous downward trajectory prior to the accident. But what the prospective data shows is something different: individuals with prior history who are asymptomatic at the time of the collision show collision-specific increases in pain and disability that exceed both their pre-collision baseline and what would be predicted by vulnerability alone.
In other words, the collision is doing something. The prior history is predicting how much it does — not whether the collision matters.
This is the essence of probabilistic clinical reasoning. We are not saying: “You had prior back pain, so this accident didn’t affect you.” We are saying: “You had prior back pain, which is why this accident affected you more than it would have affected someone without that history — and why your recovery requires more careful attention and more sustained follow-up than a first-episode patient.”
These are very different clinical and legal conclusions. And confusing them has real consequences for patients.
“Precision about uncertainty is something quite different from imprecision.”
Medicine in the Language of Probability — Why Certainty Is the Wrong Ask
One of the most common frustrations in clinical practice — for both patients and clinicians — is the mismatch between what patients want to hear and what medicine can honestly say.
Patients want certainties. “Will I fully recover?” “How long will this take?” “Is the damage permanent?” These are natural questions for people whose lives have been disrupted by pain they didn’t choose.
But medicine, done honestly, operates in probabilities. And this is not a limitation of medicine — it is the correct epistemic posture toward a system as complex as the human body.
Consider what we know and don’t know about any individual patient’s recovery trajectory: we know the group-level statistics. We know that among patients with chronic whiplash-associated disorder who receive interdisciplinary rehabilitation, approximately 60–70% achieve significant functional improvement at 12 months (Rydstad et al., European Journal of Pain, 2010). We know that those with early indicators of central sensitization have worse average outcomes. We know that psychological co-morbidities double the risk of chronicity.
We do not know which group any specific patient will fall into. That knowledge is unavailable because the biological system — with its genetic variability, its neuroplasticity, its immune dynamics, its psychosocial context — is irreducibly complex. No imaging study, no blood test, no clinical assessment can predict with certainty what any individual’s nervous system will do over the next twelve months.
What we can do is assign probabilities. And act on those probabilities.
A patient with prior low back pain, early cold allodynia, high pain catastrophizing scores, and limited social support has a high probability — not a certainty — of developing chronic symptoms. That probability justifies earlier, more intensive intervention. It justifies closer follow-up. It justifies coordinating psychological support alongside physical treatment. Not because we know they will become chronic, but because the probability is high enough that acting as if they might is the responsible clinical choice.
This is what probabilistic medicine looks like in practice. It is not vagueness or hedging. It is precision about uncertainty — which is something quite different from imprecision.
The Clinical Implications — Preventative Strategies and Follow-up Protocols
Early risk stratification. The most important clinical implication of the recurrence research is that risk stratification should happen at the first post-collision visit, before patterns of chronicity have had time to establish. Tools like the STarT Back Screening Tool, the Whiplash Activity and Participation List (WAL), and quantitative sensory testing allow clinicians to assign patients to low, medium, and high risk categories based on measurable baseline factors — prior pain history being among the most important.
High-risk patients receive more aggressive early intervention: higher visit frequency, earlier psychological co-management, earlier referral for pain neuroscience education. Low-risk patients receive appropriate care without over-medicalization. This differentiation is what probabilistic reasoning makes possible — and what undifferentiated treatment protocols make impossible.
Structured follow-up at defined intervals. One of the clearest implications of the recurrence data is that discharging patients to “as needed” visits is not an appropriate clinical endpoint for those with prior pain history. A patient with documented prior low back pain who has responded well to initial treatment is not a recovered patient — they are a patient at elevated recurrence risk who has achieved a functional interim state.
The evidence base for this is directly analogous to what oncologists have long understood: a patient who responds to treatment is not cured. They are in remission, and they require structured surveillance. In musculoskeletal medicine, this means scheduling follow-up visits at three, six, and twelve months after discharge for patients with prior pain history — not because problems are expected, but because the probability is elevated enough that not monitoring would be clinically negligent. If follow-up shows continued function and no recurrence, that data point itself is clinically valuable. If it shows early recurrence, intervening at that stage rather than waiting for full symptom re-establishment produces substantially better outcomes.
Pain neuroscience education calibrated to probability. Research by Moseley and Butler has demonstrated that pain neuroscience education (PNE) reduces fear-avoidance behavior, decreases catastrophizing, and improves physical performance in chronic pain populations. For the patient with prior LBP who has recently experienced a collision, PNE delivered early — before catastrophizing has entrenched — produces better outcomes than PNE delivered after chronic patterns are established.
PNE for the probabilistic patient includes explaining the concept of a sensitized nervous system: why a prior episode of pain has altered the gain setting on the spinal cord’s pain processing, why this makes the body more reactive to the same inputs, and what the patient can actively do to modulate that gain. It also includes reframing the concept of recurrence — not as failure or proof of serious damage, but as a predictable expression of a sensitized system that can be managed effectively if caught early.
Documenting the probabilistic basis for ongoing treatment. In personal injury contexts, when treatment recommendations are based on statistical recurrence risk — not just current symptoms — those recommendations must be documented in a way that explains the reasoning. A clinician who has documented the prior pain history, the recurrence probability data, and the specific way that probabilistic risk justifies ongoing monitoring can defend that treatment plan on its scientific merits when challenged by insurers or defense counsel.

The Legal Dimension — Probability, Causation, and the Thin Skull
In personal injury medicine, the probabilistic nature of post-collision recurrence creates a specific challenge for causation arguments.
The defense position is predictable: “This patient had prior low back pain, therefore the accident didn’t cause their current complaints — those are just a continuation of a pre-existing condition.”
This argument misunderstands probability in the same way that a gambler misunderstands expected value. It treats prior history as if it were a sufficient explanation for current symptoms, when what it actually is is a risk factor that modifies outcome probability.
Here is the correct probabilistic framing: a patient with no prior LBP who experiences a rear-end collision has a baseline probability of developing chronic low back pain. A patient with prior LBP who experiences the same collision has a substantially elevated probability of the same outcome. The prior history does not explain the outcome away — it changes the probability of the outcome.
When that higher-probability outcome actually occurs, the collision is still the precipitating event. The prior history is the context that determined the magnitude of the effect. Both can be true simultaneously, and conflating them is a logical error — not a medical finding.
This is what the eggshell plaintiff doctrine captures in legal terms: the defendant takes the plaintiff as they find them. A plaintiff with elevated recurrence risk who develops chronic pain after a collision they did not cause is not “just experiencing their pre-existing condition.” They are experiencing the probabilistically predictable consequence of having their elevated-risk system subjected to a traumatic event.
“Defendants are not entitled to a plaintiff with a pristine spine.”
Humility as a Scientific Virtue
There is a broader point embedded in all of this, and it is worth stating plainly.
The demand for certainty in medicine is understandable. Patients want certainties because they are frightened. Insurers prefer certainties because certainties are cheaper to adjudicate. Attorneys want certainties because they are easier to argue. And clinicians — human beings with the natural desire to reassure — are sometimes tempted to offer them.
But the willingness to say “I don’t know for certain — I know the probability” is not weakness. It is the epistemological stance that separates scientific medicine from the long history of confident nonsense that preceded it. Medicine has caused enormous harm in the name of certainty: certain that imaging findings explained pain, certain that prior pain history invalidated current injury, certain that a clean X-ray meant nothing was wrong.
Embracing probability is not an admission of ignorance. It is an acknowledgment that the human body is a complex, adaptive, nonlinear biological system that does not yield to simple cause-and-effect narratives — and that the honest response to that complexity is not to pretend it away, but to reason carefully within it.
The 2019 Lancet Low Back Pain Series, one of the most comprehensive reviews of the field ever produced, opened with an explicit challenge to the clinical culture of false certainty: it called for medicine to “recalibrate” its approach to low back pain by acknowledging the probabilistic nature of outcomes, abandoning diagnostic labels that imply more precision than the evidence supports, and treating uncertainty as a normal feature of the clinical encounter rather than something to be resolved by yet more testing.
That recalibration is what good science looks like. And it begins with the willingness to say: I know the probabilities. I cannot give you the certainty. And the probabilities tell us something important about what we should do next.
Conclusion: The Guarantee I Can Actually Give
So when the patient turns back at the door and asks “I’m going to be okay, right?” — what do I actually say?
I say: I can’t guarantee the future. But I can tell you that the research gives us real information about what your nervous system is likely to do, based on your history and how you’re presenting right now. That information tells me we need to be more careful with you than we would be with someone who has never had back pain before. It tells me we should monitor you for longer, intervene earlier if anything changes, and give your nervous system the support it needs to recalibrate from a sensitized state.
I can tell you that patients in your situation who receive attentive, probability-informed care do significantly better than patients who get discharged with reassurance and told they’ll be fine.
I can tell you that humility about what we don’t know is not the same as helplessness about what we can do.
That’s the guarantee I can actually give. It is less satisfying than a yes. It is also true. And in medicine, as in science, the truth — however probabilistic — is always the better starting place.
