Move More to Protect Your Spine: What I Brought Home from Parker Seminars Las Vegas
Last week I was at Parker Seminars in Las Vegas, sitting in a room full of clinicians while the presenter walked through something that should change the way many people think about pain, stability, and exercise.
Here is the big takeaway I want you to carry with you:
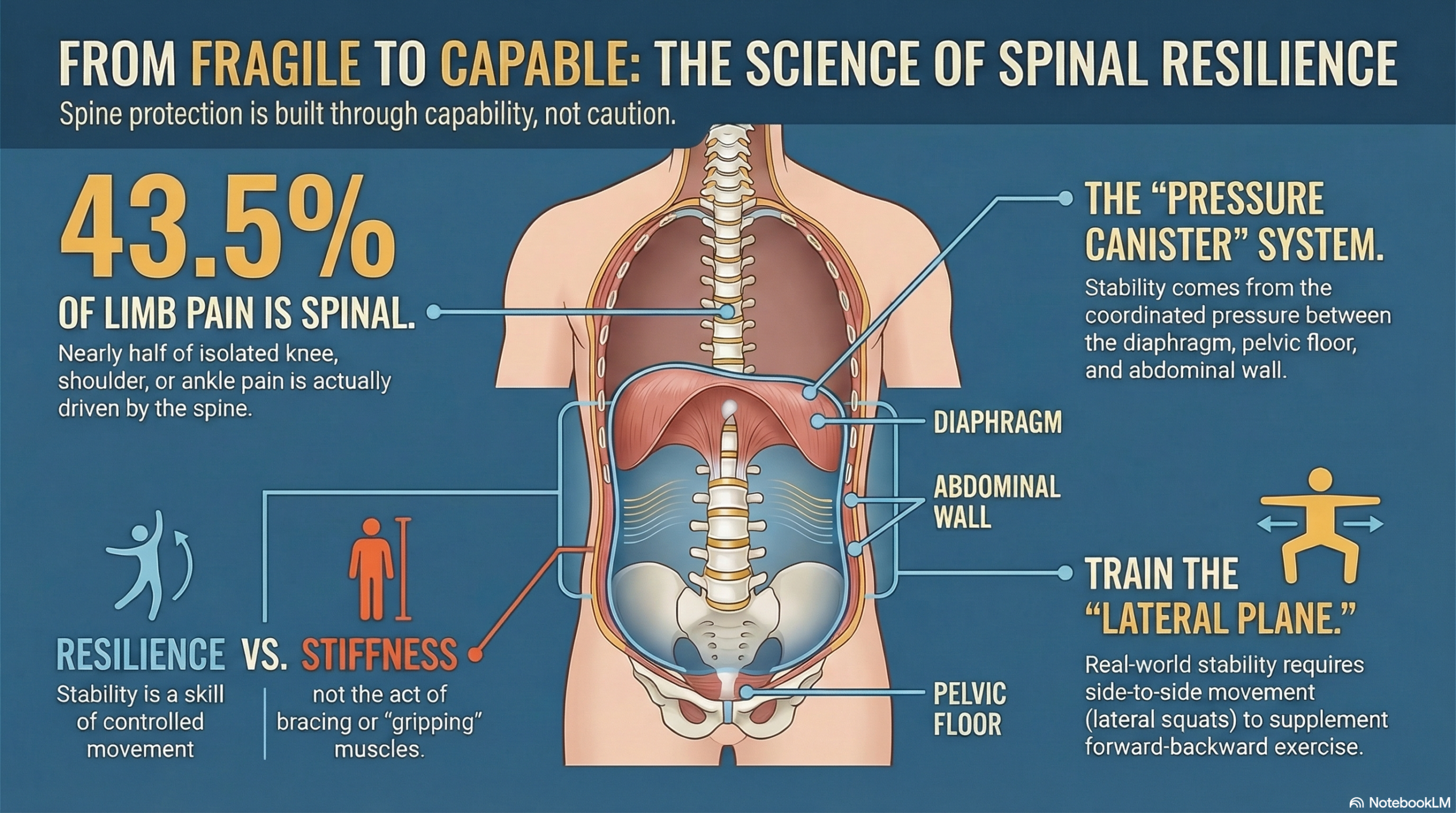
"Your spine is not protected by being careful. Your spine is protected by being capable."
— Dr. Todd Lloyd, D.C.
Capability is built through the right kind of movement, practiced consistently, progressed patiently, and anchored in good mechanics and good breathing. And yes, that includes people who are in pain. It includes people who have had car accidents. It includes people who have been told their scans are “normal” while their symptoms are very real.
This post is for my patients, and for anyone trying to make sense of stubborn pain, recurring flare-ups, or that uneasy feeling that your body is “fragile.” I want to show you a few ideas from Parker Seminars, connect them to real life, and give you a simple way to start building spinal stability through physical activity.
Sometimes the Pain Is in Your Arm or Leg, but the Source Is Your Spine
One of the most striking pieces of information that came up at Parker was this:
43.5%
of patients with isolated extremity pain had a spinal source of symptoms
Let that sink in. Almost half of the people who were confident their pain was “in the knee,” or “in the shoulder,” or “in the ankle,” had symptoms that were being driven by the spine.
Why this matters to you
If you have pain that keeps coming back, changes location, feels “out of proportion” to what you did, does not match what your imaging says, improves briefly with local treatment and then returns, or comes with neck or low back stiffness, there is a real possibility the spine is involved in the “wiring,” the sensitivity, or the mechanics of what you are feeling.
This does not mean your pain is “all in your head.” It means your body is an integrated system. The spine can refer symptoms. The nervous system can amplify. And movement patterns can load one area while the brain perceives the problem somewhere else.
Key Takeaway
If we only chase the symptom location, we can miss the driver. A good recovery plan often includes assessing the spine even when symptoms show up in the arm or leg.
Spinal Stability Is Not Stiffness. It Is Control.
A lot of people think “spinal stability” means a tight core, rigid posture, bracing all day, and avoiding bending, lifting, and twisting.
But what I want for you is not a spine that is rigid. I want a spine that is resilient.
Resilience looks like control. It looks like moving through ranges without fear, breathing without tightening your neck and jaw, carrying, squatting, stepping, pushing, pulling, and rotating without your body panicking, and recovering after activity instead of collapsing into a flare-up.
Stability is a skill. Skills are trained.
And training requires movement.
Why Breathing and Posture Matter: The “Pressure Canister”
One of the best visuals from Parker was how posture changes the orientation of your diaphragm and pelvis, and how that affects the way your trunk stabilizes.
You can think of this as a “pressure canister.” Your diaphragm is the top. Your pelvic floor is the bottom. Your abdominal wall and back muscles form the sides. When those parts work together, they create intra-abdominal pressure, which is one of your body’s most important stability tools.
When the system is off, the body often tries to substitute with “gripping” strategies, like neck tension, rib flare, shallow breathing, overactive low back muscles, clenching glutes all day, or bracing that never turns off.
In other words, the body tries to create stability through tension instead of coordination.
Did You Know
If you feel like you “can’t take a deep breath” when your neck or low back flares up, that is often a sign your stability system is defaulting to guarding instead of coordination.
A Simple Progression: Train Breathing Where It Is Easier, Then Stand Up
A smart rehab principle is to start with positions where compensation is minimized, train the pattern, and then gradually load it. That same logic applies to breathing and stability.
What this can look like
- Phase 1 (easy): Breathing practice lying on your back with knees bent
- Phase 2 (better alignment): Breathing in a 90/90 position (hips and knees bent, feet supported)
- Phase 3 (challenge): Breathing while one leg moves (asymmetric demand)
- Phase 4 (transfer): Breathing seated or standing, then during exercise
The point is not to become a professional breather. The point is to restore coordination between breath and stability so movement stops feeling like a threat.
Why Side-to-Side Strength Matters: The Lateral Squat Lesson
Most people’s exercise lives happen in one plane: forward and backward. Walking forward. Squatting up and down. Lunging forward. Sitting down and standing up.
But real life is not only forward. You step sideways. You catch yourself. You rotate. You reach. You carry something awkward. You get bumped. You slip a little.
Your spine has to stay stable through all of it.
One movement that came up at Parker was the lateral squat (a side-to-side squat and lunge pattern). The reason it matters is simple: it trains frontal-plane control. That is the kind of control your body needs for hip stability, knee tracking, ankle control, pelvic control, and spinal stability.
Key Takeaway
Getting stronger only “straight ahead” can still leave you feeling unstable in real life. Adding gentle lateral training is one way to build practical stability.
If You Are in Pain, Read This Before You Quit Moving
If you are thinking, “This sounds great, but I can’t work out because I’m in pain,” I want to address that directly.
Here is a pattern I have seen for years: someone gets hurt (often after a car accident). They rest. They become cautious. The body becomes guarded. They move less. They lose capacity. Then normal activity feels threatening, because it is threatening to a body that is no longer trained for it.
That is not a character flaw. That is physiology.
The goal is not to “push through pain.” The goal is to rebuild capacity without constantly triggering the alarm system.
The goal is not to be fearless. The goal is to be capable.
What Physical Activity Does for Spinal Stability (In Plain Language)
If you want better spinal stability, physical activity helps by improving several key things.
1) Endurance and coordination
Stability is more about endurance than max strength. You want the ability to hold alignment and control for minutes and hours, not just for a single rep.
2) Tissue tolerance
Tendons, ligaments, discs, and joints adapt to load. The right amount of progressive load teaches tissues that movement is safe again.
3) Nervous system confidence
Your brain learns through exposure. If all your exposure is avoidance, your nervous system learns “danger.” If your exposure is progressive, controlled movement, it learns “capable.”
4) Breathing mechanics under load
It is one thing to breathe well lying down. It is another to breathe well carrying groceries, walking up stairs, or lifting your kid. Training is how that transfer happens.
5) Recovery capacity
Active bodies recover faster. This matters for spinal stability because people who recover well can tolerate life. People who do not recover well often get more cautious, and caution can quietly become deconditioning.
How to Start This Week (Without Sabotaging Yourself)
If you want a starting point that works for most people, here is what I recommend.
Step 1: Pick a base activity you can do 4–6 days per week
This is not about hero workouts. This is about consistency. Start with what you can do without paying for it with a flare-up.
- Walking
- Stationary bike
- Gentle hiking
- Swimming
- Light strength training circuit
- Mobility work with a little heart rate
Step 2: Add two days of simple strength (10–25 minutes)
Your goal is not exhaustion. Your goal is patterning and capacity.
- Squats to a chair
- Hip hinges (bodyweight, dowel, or light weight)
- Step-ups
- Rows or band pulls
- Loaded carries (even grocery bags count)
- Side steps with a band
Step 3: Add one lateral movement pattern
You do not need advanced lateral squats on day one. Start shallow and controlled.
- Side step-downs
- Lateral lunges to a shallow depth
- Cossack squat progression (very shallow at first)
- Banded lateral walks
Step 4: Use breathing as a tool, not a ritual
If breathing drills help you calm down and move better, use them. But breathing is a bridge to movement, not a replacement for movement.
Important
If you have new numbness, progressive weakness, loss of balance, bowel or bladder changes, fever, unexplained weight loss, or severe night pain, get medical evaluation right away before starting a new exercise plan.
The Two Most Common Mistakes I See
Mistake 1: Doing too much too soon
A good rule: if you are not sure, start about 30% easier than you think. Then build. Stability is built through repeat exposures the body can tolerate.
Mistake 2: Waiting for “zero pain” before moving
Most people do not get to zero pain by waiting. They often get there by rebuilding capacity so the nervous system does not need to protect as much. If the body only moves when it feels perfect, it rarely learns to feel safe.
How to Know You Are on the Right Track
Progress usually looks like this:
- Fewer “random” flare-ups
- Faster recovery after activity
- Improved sleep
- Less guarding through the neck, jaw, and shoulders
- More confidence bending, lifting, and carrying
- Better tolerance to sitting and driving
- Less need for constant self-protection strategies
And here is the most important one: you start to feel like your body is yours again.
My Ask for You This Week
If you take nothing else from this post, take this:
Try This
Pick one form of physical activity you can do this week, and do it three times. The goal is not intensity. The goal is consistency.
It could be a 15-minute walk. It could be a light strength circuit. It could be a mobility routine plus a short bike ride.
The goal is a message to your nervous system: “I’m not fragile. I’m rebuilding.”
If you are a patient in my office and you want help choosing the right starting point, that is what we do. We look at the pattern, we test what changes your symptoms, and we build a plan that restores stability through progressive movement without constantly triggering the system.
Because the end game is not “being careful.” The end game is getting your life back.
