There is a moment in many collision cases I treat — somewhere around visit three or four — when the patient says something that stops me. It is not a complaint about stiffness or range of motion. It is quieter than that.
"My shirt hurts my skin."
"I flinched when my daughter hugged me."
"The seatbelt touched my shoulder and I almost screamed."
These are not exaggerations. They are not symptoms of anxiety, and they are not signs that something has been "missed" on imaging. They are evidence that the nervous system has done exactly what it was designed to do after physical trauma: it shifted its thresholds.
Over the past four years, I have treated more than a thousand personal injury cases. I have watched this pattern repeat with startling consistency. A rear-end collision at 8 mph. A "minor" fender-bender in a parking lot. The vehicle barely dented. And yet the patient sitting across from me cannot tolerate a light touch to the trapezius. The disconnect between what the outside world sees (a small accident, a clean MRI) and what the patient feels (searing pain from a gentle hand) is one of the most misunderstood phenomena in post-traumatic care.
The science, however, is not confused at all. The nervous system recalibrates after trauma. What was once innocuous becomes threatening. What was once background noise becomes an alarm. And understanding how and why this happens is the first step toward helping someone find their way back.
This article is built on that premise. Not as opinion, but as biology — grounded in peer-reviewed research from the fields of pain science, neurology, and rehabilitation. If you have ever wondered why your pain seems "out of proportion" to your injury, or why a patient reacts as though you have struck them when you have barely pressed, the answer lives in the mechanisms we are about to explore.
The Architecture of Normal Pain Processing
Before we can understand what changes after trauma, we need to understand what the system looks like when it is working normally.
Pain is not a simple input-output event. You do not stub your toe, send a signal to the brain, and receive "pain" in return like a vending machine dispensing a product. The reality is far more complex — and far more interesting.
The spinal cord dorsal horn serves as the initial integration site where somatosensory input is processed by the central nervous system. It is organized into distinct laminae, each associated with specific types of sensory information. Primary afferent fibers that transmit pain, touch, itch, and proprioceptive inputs are categorized into different types — Aα, Aβ, Aδ, and C fibers — each conveying distinct sensory modalities (Todd, 2010; Merighi, 2018). Myelinated Aβ and low-threshold Aδ fibers, which mediate innocuous mechanical sensitivity, primarily project to the deeper laminae (II inner, III, and IV). In contrast, high-threshold myelinated Aδ and unmyelinated C fibers — the ones that mediate pain and thermal sensations — mainly terminate in lamina I and II.
What this means in practical terms: your nervous system has a sorting mechanism. Light touch goes to one set of mailboxes. Noxious, potentially damaging stimulation goes to another. The thresholds that determine which signals get routed where are set by your neurological history, your current state of arousal, and — critically — whether you have recently experienced tissue injury.
In a healthy, uninjured state, these thresholds are calibrated so that ordinary life does not hurt. The pressure of clothing against skin, the vibration of a car seat, the stretch of turning your head — these inputs are processed, categorized as non-threatening, and largely ignored by conscious awareness.
Trauma changes the calibration.

Central Sensitization: When the Alarm System Recalibrates
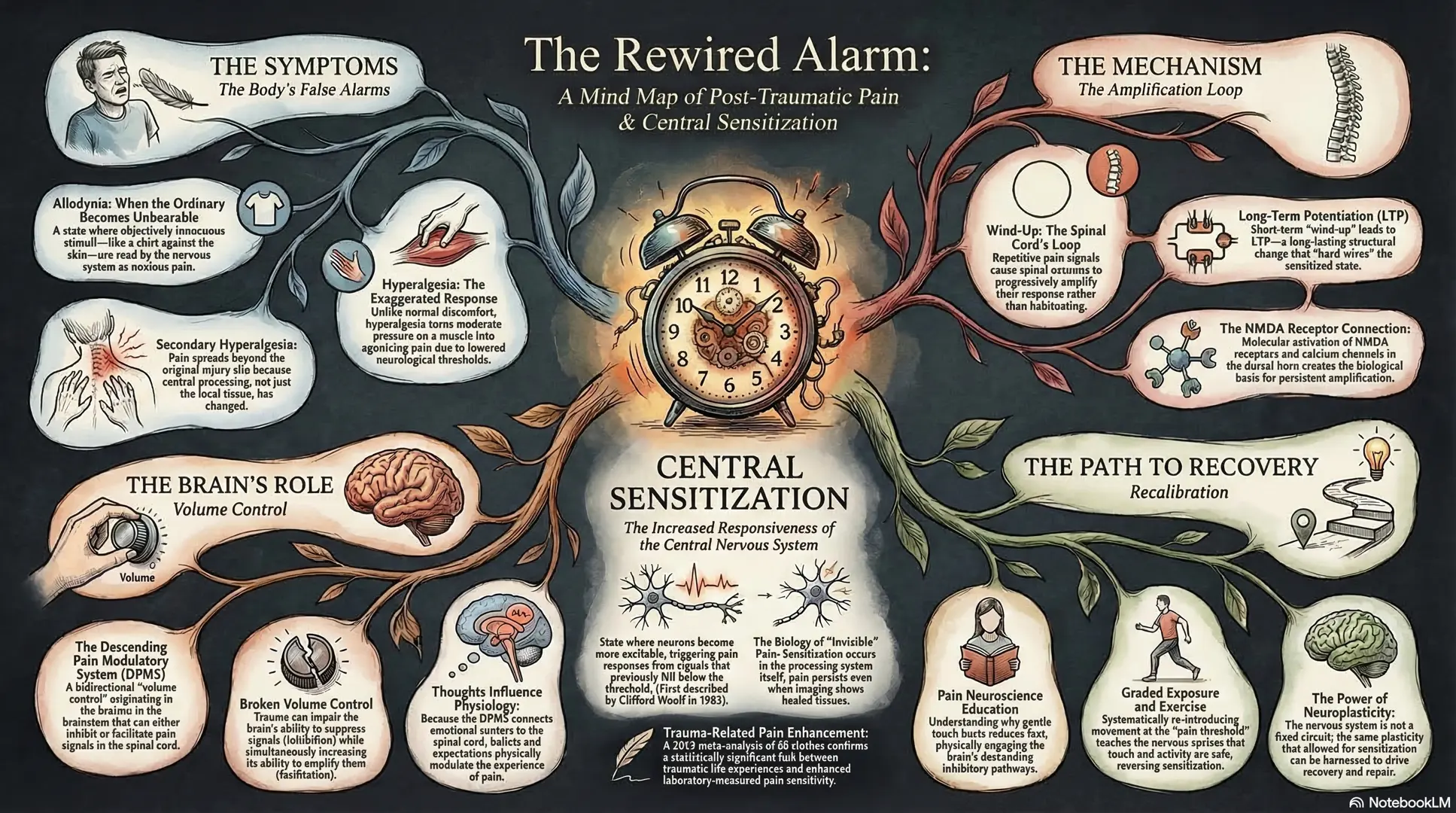
The phenomenon at the heart of post-traumatic pain amplification has a name: central sensitization.
Clifford Woolf, who first described the mechanism in 1983, defines it as "an increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold afferent input" (Woolf, 2011). In plain language: the neurons that process pain become more excitable. Signals that previously fell below the threshold for triggering a pain response now exceed it.
This is not a peripheral problem. It is not that the tissues are more damaged than imaging suggests. It is that the processing system itself has changed its settings.
Key finding: A 2023 meta-analysis of 48 studies (147 effect sizes) found a statistically significant association between traumatic life experience and enhanced laboratory pain sensitivity (g=0.24, P=0.0002). The relationship was driven by effects on pain detection thresholds (g=0.28) and central sensitization markers (g=0.22). — You et al., Clin J Pain, 2023
Woolf's landmark review in Pain (2011) demonstrated that central sensitization manifests clinically as pain hypersensitivity — particularly dynamic tactile allodynia, secondary punctate or pressure hyperalgesia, aftersensations, and enhanced temporal summation. He showed that this state can be "readily and rapidly elicited in human volunteers by diverse experimental noxious conditioning stimuli to skin, muscles or viscera" and produces secondary changes in brain activity detectable by electrophysiological and imaging techniques.
Curatolo's 2024 review in Current Rheumatology Reports reinforced this understanding, noting that central sensitization has measurable, objective correlates — not merely subjective complaints.
For anyone who has had their pain dismissed because their imaging looked clean, this research is validation. The problem is real. It is measurable. And it has a mechanism.

Wind-Up: The Spinal Cord's Amplification Loop
Central sensitization does not appear from nowhere. One of its key precursors is a phenomenon called wind-up — a progressive, frequency-dependent increase in the excitability of spinal cord neurons.
Herrero, Laird, and Lopez-Garcia published a comprehensive review in Progress in Neurobiology (2000) describing wind-up as a facilitation of neuronal responses observed when repetitive stimuli of constant intensity are applied to C-fiber afferents. The same stimulus, delivered repeatedly, produces a progressively larger response in the dorsal horn. The neuron does not habituate; it amplifies.
The mechanism involves NMDA receptor activation, L-type calcium channel engagement, and a synaptic balance between excitatory and inhibitory inputs. When repetitive nociceptive C-fiber stimulation occurs — as it does during and after a motor vehicle collision — NMDA receptors on dorsal horn neurons are activated. This opens calcium channels, increases intracellular calcium, and produces a progressively amplified response to each successive input.
From short-term to structural: Wind-up is technically a short-lived process. But repetitive episodes can precipitate long-term potentiation (LTP) — a long-lasting increase in synaptic efficacy that alters synaptic plasticity. Both wind-up and LTP are believed to be important components of central sensitization. This is how a collision that lasts less than a second can produce pain that lasts months or years.
Recent molecular work has even identified specific genetic contributors. A 2022 study in Neuron found a significant genetic association between human pain wind-up and the NCX3 locus (sodium-calcium exchanger-3). Mice lacking NCX3 showed hypersensitivity in inflammatory and neuropathic pain models, while their dorsal horn neurons exhibited increased wind-up and intracellular calcium. Viral overexpression of NCX3 in the spinal cord reduced pain-related behavior — suggesting that calcium efflux capacity is a concrete, targetable biological variable.
This is how a collision that lasts less than a second can produce pain that lasts months or years. The initial tissue injury generates a barrage of nociceptive input. That input drives wind-up. Repeated wind-up drives LTP. And LTP contributes to a sensitized central nervous system that now interprets ordinary sensations as threatening.

Allodynia and Hyperalgesia: When the Ordinary Becomes Unbearable
The clinical consequences of central sensitization have specific names that every collision patient — and every attorney handling such a case — should understand.
Allodynia is pain produced by a stimulus that does not normally cause pain. A shirt against the skin. A seatbelt across the chest. A light touch during examination.
Hyperalgesia is an exaggerated pain response to a stimulus that would normally cause only mild pain. Pressing on a sore muscle should produce discomfort, not agony. In a hyperalgesic state, moderate pressure produces severe pain.
Secondary hyperalgesia involves a receptive field expansion — the area of sensitivity spreads beyond the site of original injury. A patient injured in the cervical spine begins reporting pain in the thoracic region, the shoulders, the hands. This expansion is not evidence of additional structural injury. It is evidence that central processing has changed.
When gentle touch produces real pain, your nervous system is not lying. It has shifted its thresholds.
These phenomena are extensively documented in whiplash populations. Curatolo and colleagues (2001) were among the first to explicitly connect whiplash with central hypersensitivity, demonstrating measurable changes in how the nervous system processes sensory information after cervical injury. Sterling and colleagues (2009) documented the full sensory profile: elevated detection thresholds in some modalities occurring simultaneously with hypersensitivity in others — a paradoxical pattern that reflects the complexity of nervous system recalibration.
Bock and colleagues (2005) documented thoracic allodynia in a whiplash cohort, observing that patients with cervical injuries frequently presented with widespread mechanical allodynia in areas remote from the injury site — consistent with central sensitization rather than peripheral tissue damage.
Here is what I want you to understand if you are a patient reading this: when gentle touch produces real pain, your nervous system is not lying. It has shifted its thresholds. The alarm is going off at a lower setting — not because you are broken, but because your biology is trying to protect you.

The Descending Modulation System: The Brain's Volume Control
If central sensitization turns the volume up, the brain has a system designed to turn it back down. Understanding this system is essential to understanding recovery.
The descending pain modulatory system (DPMS) comprises neuronal pathways that originate in the brainstem and project downward to the spinal cord, where they modulate dorsal horn neuron activity. This system is bidirectional — it can both inhibit and facilitate pain signaling (Heinricher et al., 2009).
The key relay stations include the periaqueductal gray (PAG), the rostral ventromedial medulla (RVM), the anterior cingulate cortex (ACC), and the amygdala. These structures form a circuit connecting higher cognitive and emotional brain regions with the spinal cord — providing a mechanism through which thoughts, beliefs, expectations, and emotions can genuinely influence the experience of pain.
This is not a metaphor. It is neuroanatomy.
A 2024 review in JOSPT by Nijs and colleagues explained that the DPMS provides the mechanistic basis for understanding why counter-stimulation techniques (acupuncture, manual therapy), patient expectations and beliefs, and social or contextual factors all influence pain perception.
The double hit: A study in Pain Medicine found that trauma exposure disrupts cerebrospinal inhibition of spinal nociception. Trauma does not just amplify incoming signals through central sensitization — it simultaneously impairs the brain's ability to suppress those signals through descending inhibition. The alarm is louder and the volume control is broken. — Penza et al., 2018
Descending facilitation — the system's ability to amplify rather than suppress pain — has attracted significant research attention. A review in Molecular Pain (2017) described how brain activity can directly enhance sensory transmission through facilitatory pathways from the RVM to the spinal cord, and that this facilitation plays a role in the chronification of pain.
This explains one of the most frustrating experiences for collision patients: the MRI is clean, the fracture has healed, the soft tissue should have recovered — and yet the pain continues. The source of that pain is not in the tissues. It is in the processing system. The descending modulatory balance has not yet been restored.

From Sensitization to Chronification: What Determines Who Gets Stuck
Not everyone who experiences central sensitization after trauma develops chronic pain. The question of who recovers and who gets stuck is one of the most important in post-traumatic care.
A 2025 scoping review on central sensitization after orthopaedic trauma found that a substantial subgroup of trauma patients progress to chronic pain with centrally mediated features. Neuropathic pain descriptors were reported in up to one-third of patients following major trauma and were associated with greater disability and poorer quality of life.
The early predictors are striking: severe acute pain, high opioid exposure without multimodal strategies, catastrophizing, sleep disturbance, and PTSD symptoms — all linked to adverse long-term outcomes.
Notice what is on that list and what is not. Vehicle damage is not on the list. Imaging findings are not on the list. What predicts chronification is the neurobiological response to injury.
The Cleveland Clinic's 2023 review made this point directly: "When patients have chronic pain or other symptoms that seem out of proportion to anything we can tell is physically wrong with them, we should not assume they are faking it. The central nervous system can undergo changes — structural, functional, and chemical — that make it more sensitive to stimuli."
When patients have chronic pain that seems out of proportion to anything physically wrong, we should not assume they are faking it.
A fascinating counterpoint comes from Dar, Ariely, and Frenk (1995), who found that severely injured military veterans had higher pain thresholds than lightly injured veterans. Recalibration is not always in the direction of sensitization. The direction depends on context, chronicity, psychological processing, and the nature of the trauma itself.

Recovery as Recalibration
If trauma shifts the nervous system's thresholds downward — making it more reactive, more protective, more amplified — then recovery must involve shifting them back. Not to a state of numbness or denial, but to a state where the system accurately distinguishes between genuine threat and ordinary sensation.
Pain Neuroscience Education
Patient education about pain physiology and central sensitization has been shown to improve quality of life and functional status, and to reduce anxiety and catastrophization (Nijs et al., CCJM, 2023). When patients understand why gentle touch hurts — when they grasp that the alarm is misfiring rather than accurately reporting tissue damage — it changes their relationship to the pain. It reduces fear. It enables engagement with rehabilitation. It restores agency.
This is not a soft intervention. It is a neurobiological one. Education changes expectations, and expectations modulate descending inhibitory pathways.
Graded Exposure and Exercise
Because the nervous system has learned to interpret certain stimuli as threatening, recovery involves systematically re-introducing those stimuli at tolerable levels and progressively increasing intensity. Research on pain-threshold rehabilitation shows better structural and functional outcomes compared to pain-free approaches — working at the threshold, not avoiding it, produces superior recovery (Hickey et al., 2020).
Manual Therapy
Lowry and colleagues (2010) documented the resolution of whiplash-associated allodynia following cervicothoracic manipulation. Manual therapy generates afferent input that engages descending inhibitory pathways, modulating the processing — not just the tissues.
This is why chiropractic manipulation can produce immediate pain relief that seems disproportionate to the mechanical forces involved — it is modulating the processing, not just the tissues.
Neuroplasticity: The Biological Basis of Hope
The nervous system is not a fixed circuit. A 2025 review on neuroplasticity described the nervous system's ability to "adapt structurally and functionally in response to environmental interactions and injuries" as a cornerstone of recovery. The same plasticity that drove sensitization can drive recovery.
Clinical Pacing: The Art of Not Rushing
One of the most important clinical lessons I have learned is that recovery from sensitization cannot be rushed. Pushing too hard, too fast, re-triggers the protective response and reinforces the very sensitization you are trying to reverse. The art is in finding the edge — the boundary between productive challenge and re-injury — and working there with patience and precision.

Conclusion
The nervous system does not sensitize out of malice. It lowers its thresholds because, in the aftermath of trauma, protection is more important than accuracy.
Central sensitization is not a life sentence. The same neuroplasticity that shifted your thresholds downward can shift them back. The same dorsal horn neurons that amplified your pain can be retrained. The same descending modulatory pathways that lost their inhibitory capacity can be re-engaged through education, graded exposure, manual therapy, and time.
Recovery is not the absence of pain. It is the restoration of accurate signaling — a nervous system that once again distinguishes between what is dangerous and what is not. It is a process of re-calibration.
And if there is one thing I have learned in over a thousand cases, it is this: the body wants to recalibrate. It wants to return to accurate processing. Our job — as clinicians, as patients, as human beings navigating the aftermath of trauma — is to create the conditions that allow it to do so.
References
- Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2-S15. PMID: 20961685
- You DS, et al. Traumatic life experience and pain sensitization: meta-analysis of laboratory findings. Clin J Pain. 2023;39(3):138-149. PMID: 36524769
- Curatolo M. Central sensitization and pain: pathophysiologic and clinical insights. Curr Rheumatol Rep. 2024. PMID: 36237158
- Herrero JF, Laird JM, Lopez-Garcia JA. Wind-up of spinal cord neurones and pain sensation. Prog Neurobiol. 2000;61(2):169-203. PMID: 10704997
- Curatolo M, et al. Central hypersensitivity in chronic pain after whiplash injury. Clin J Pain. 2001;17(4):306-315. PMID: 11783810
- Sterling M, et al. Characterization of acute and chronic whiplash-associated disorders. J Orthop Sports Phys Ther. 2009. Full text
- Bock S, et al. The presence and interrater reliability of thoracic allodynia in a whiplash cohort. Pain Physician. 2005;8:267-270.
- Heinricher MM, et al. Descending control of nociception: specificity, recruitment and plasticity. Brain Res Rev. 2009;60(1):226-242. PMC4301419
- Dar R, Ariely D, Frenk H. The effect of past-injury on pain threshold and tolerance. Pain. 1995;60(2):189-193. PMID: 7784104
- Lowry CD, O'Hearn MA, Courtney CA. Resolution of whiplash-associated allodynia following cervicothoracic manipulation. Physiother Theory Pract. 2010. PMID: 20977379
- Nijs J, et al. Central sensitization, chronic pain, and other symptoms: better understanding, better management. Cleve Clin J Med. 2023;90(4):245-258. Full text
- Penza CW, et al. Conditioned pain modulation in sexual assault survivors. Pain Med. 2018. PMC6711837
- Neuroplasticity and nervous system recovery: cellular mechanisms, therapeutic advances, and future prospects. 2025. PMC12025631
- Hickey JT, et al. Pain-free vs pain-threshold rehabilitation following acute hamstring strain injury. J Orthop Sports Phys Ther. 2020;50(2):91-103. Full text