Stability as Tolerance: Why the Body’s True Strength Is Its Capacity to Absorb What the World Throws at It
Why true resilience isn’t rigidity—and why rebuilding your body after injury means learning to absorb force, not resist it.
Introduction: The Word We’ve Been Using Wrong
When a patient walks into my office after a motor vehicle collision and tells me they want to “build stability” in their spine, I know what they mean. They want to feel strong again. Safe. They want a body that won’t betray them the next time something goes wrong.
I know what you’re thinking too, probably: stability means being solid. Held in place. Resistant to movement.
Here’s what’s actually happening in a well-functioning body: none of that is true.
In twenty-five years of chiropractic practice—and across more than a thousand personal injury cases in Sonoma County over the past four years—I have watched patients pursue the wrong version of stability with tremendous dedication. They brace. They guard. They strengthen the muscles that are already overworking. They become, in the most literal sense, armored.
And then they get hurt again. Or they plateau in recovery and can’t understand why. Or they return to activity only to find their body stiff, reactive, and still afraid of the forces that daily life demands of it.
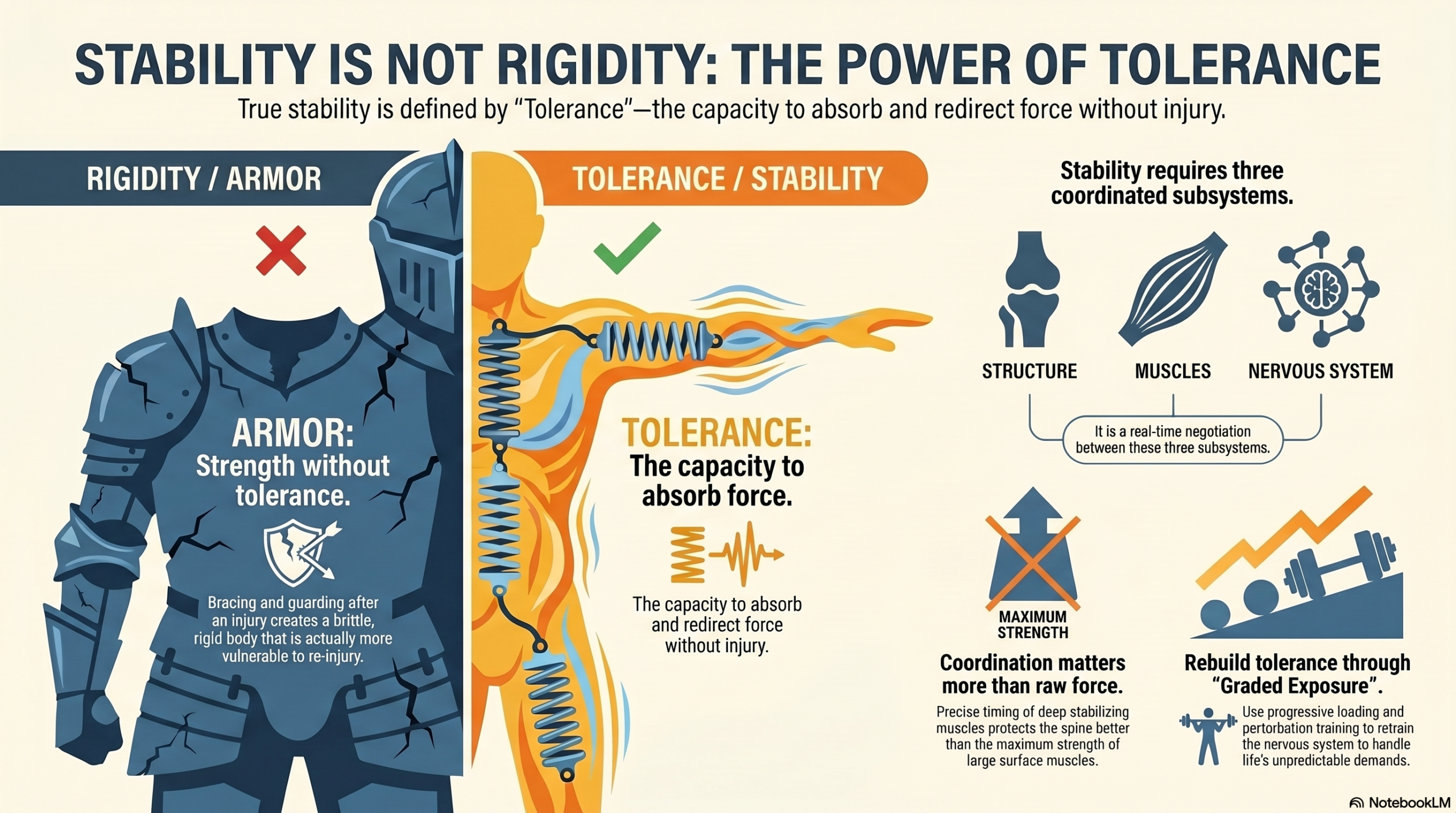
The problem is the model. We have been thinking about stability as a property of position—as the body’s ability to stay put. The science tells a different story entirely. True stability is not rigidity. It is tolerance. It is the capacity of the musculoskeletal and nervous system to absorb, manage, and recover from forces without losing control or sustaining injury.
Strength without tolerance is just armor. And armor is heavy, brittle, and ultimately not what the body needs.
This essay is about what stability actually means, why tolerance—not stiffness—is the defining quality of a resilient body, and what that means for recovery from personal injury.
Section 1: Rethinking Stability — From Position to Capacity
In classical biomechanics, stability has historically been defined in structural terms: a structure is stable when it resists displacement from its equilibrium position. Think of a pyramid—wide base, low center of mass, resistant to toppling.
For a building, this is a reasonable model. For a living body that must run, twist, lift, catch itself mid-fall, absorb the impact of a collision, and perform a thousand unpredictable movements every day, it is profoundly inadequate.
The landmark work of Panjabi (1992), published in the Journal of Biomechanical Engineering, introduced a more nuanced and biologically accurate model: the spinal stabilizing system. Panjabi proposed that spinal stability is not a fixed structural property but a dynamic function achieved through the coordinated interaction of three subsystems.
The passive subsystem consists of the vertebrae, discs, facet joints, and spinal ligaments—the structural elements that provide mechanical stiffness and set the limits of range of motion. These elements are relatively rigid, but they contribute only a portion of the total stability picture, particularly in the mid-ranges of motion where ligaments are slack and cannot provide meaningful constraint.
The active subsystem consists of the muscles and tendons surrounding the spine. These provide the dynamic, adjustable forces that stiffen and control the spine in response to changing loads. Critically, muscles can modulate their stiffness in milliseconds—far faster than conscious control allows.
The neural control subsystem is the conductor: the network of proprioceptors, mechanoreceptors, and central nervous system circuits that monitor the state of the spine, detect perturbations, and coordinate the muscular responses needed to maintain control. Without appropriate neural input, the active subsystem cannot respond correctly, no matter how strong the muscles are.
Stability, in this model, is not a static state. It is a continuously updated performance—a real-time negotiation between the forces acting on the body and the body’s capacity to absorb and redirect those forces without injury or loss of control.
Tolerance is the measure of that capacity. It is how much load the system can manage before control fails. And it is tolerance, not strength alone, that determines who recovers well from injury—and who doesn’t.
Section 2: How a Healthy Body Absorbs Force — The Neuromuscular Coordination System
You’ve experienced the body’s force-absorption system without knowing it. Walk across an uneven parking lot and your ankle subtly adjusts with every step. Catch a heavy grocery bag at an unexpected angle and your shoulder stabilizes before you consciously register the load. Drive over a pothole and your spine absorbs the vertical impact without your needing to think about it.
These are not passive events. They are rapid, coordinated neuromuscular responses executed in milliseconds by systems operating largely below conscious awareness.
The mechanics of force absorption in the healthy spine involve multiple layers of response. At the local level, deep stabilizing muscles—the multifidus, the transversus abdominis, the deep cervical flexors—are continuously active at low levels, providing what researchers call intersegmental stiffness: a baseline level of muscular pre-tensioning that keeps individual vertebral segments controlled even before any external load is applied. These muscles are not strength muscles in the traditional sense. They are precision muscles. They contribute relatively little to gross movement but are essential to the fine-grained control that prevents abnormal segmental motion.
At a global level, larger superficial muscles—the erector spinae, the rectus abdominis, the gluteal complex—respond to more substantial loads by generating the forces needed to transmit load through the kinetic chain without overwhelming any single joint or disc.
Between these two layers, neural control coordinates the timing, sequencing, and magnitude of muscular responses based on continuous sensory feedback from proprioceptors throughout the spine, pelvis, and extremities. Research by Hodges and Richardson demonstrated that in healthy individuals, the transversus abdominis activates before limb movement—before the load even arrives. This feedforward activation is not something the person consciously initiates. It is the nervous system’s anticipatory preparation for a known demand.
After injury, this feedforward mechanism is disrupted. The deep stabilizers delay. The superficial muscles compensate by activating harder and earlier. The system becomes reactive instead of anticipatory, responsive instead of prepared. The body can no longer absorb forces the way it did before—because the neural control system has been altered.
This is the core of why strength training alone does not restore stability after injury. You can make the superficial muscles stronger, and the person will be able to lift more. But if the deep stabilizing system remains delayed, and the neural feedforward mechanism remains disrupted, you have made the armor thicker without repairing the underlying coordination system.
“Strength without tolerance is just armor.”
Section 3: When Tolerance Fails — Injury and the Loss of Load Capacity
In a rear-end collision, or a slip-and-fall, or any of the sudden unexpected loads that bring patients through my door, what fails first is not usually the structure. It is the tolerance system.
The forces of a sudden collision arrive faster than the neuromuscular system can mount a protective response. The feedforward system cannot help; there was no warning. The passive structural elements—the ligaments, the disc annulus, the facet joint capsules—are loaded beyond their immediate capacity before the active muscular system can engage. The result is microtrauma: small tears in ligamentous fibers, disruption of facet joint capsule mechanoreceptors, compression injury to disc annular fibers.
The structural damage, in many cases, is real but modest. What is not modest is the effect on the tolerance system.
Mechanoreceptors in the injured facet joint capsules—which were providing a significant fraction of the proprioceptive information the neural control system relied on—are now disrupted. Their signaling becomes unreliable. The neural control system receives distorted input and cannot generate accurate feedforward or feedback responses. The deep stabilizing muscles, which depend on accurate proprioceptive input to time their activation correctly, become dysregulated.
Research by Solomonow and colleagues demonstrated that sustained or cyclic loading of spinal ligaments—even at sub-injury levels—produces a phenomenon called laxity creep: a transient increase in ligamentous laxity accompanied by a paradoxical decrease in muscular protective reflexes. The very load that should trigger protective muscle activation instead suppresses it. The tolerance system is not just damaged; it is inverted.
Meanwhile, the nervous system—interpreting the injured region as a zone of threat—increases protective muscle tone in the superficial layers. The sternocleidomastoid and upper trapezius become guarded and overactive. The deep cervical flexors and multifidus become inhibited. The body has substituted global compression and stiffening for the precise local control it can no longer access.
This pattern—deep inhibition, superficial overactivation, reduced proprioceptive fidelity, impaired feedforward timing—is the signature of reduced tolerance. And it is what makes the post-injury spine vulnerable to re-injury from forces that would previously have been absorbed without consequence.
The painful paradox is that a guarded, stiff-feeling body is not a tolerant body. The armor sensation—that protective rigidity that post-injury patients often mistake for stability—is actually a sign of reduced tolerance capacity. The body is bracing because it has lost its ability to coordinate. It is stiff because it is afraid.
The Painful ParadoxA guarded, stiff-feeling body is not a tolerant body. The armor sensation—that protective rigidity post-injury patients often mistake for stability—is a sign of reduced tolerance capacity. The body is bracing because it has lost its ability to coordinate.
Section 4: The Armor Trap — Why Strength Alone Doesn’t Restore Tolerance
I’ve treated patients who spent months after their collision doing exactly what they were told: core strengthening, shoulder presses, resistance band work. By the time they walked into my office, they were measurably stronger. Their surface muscles were well-conditioned.
They were also still in pain, still guarded, still unable to absorb the simple unpredictable demands of real life: catching a falling object, turning quickly, sitting through a two-hour meeting without their neck seizing up.
I know what you might think: Maybe they just need more strength. Maybe they didn’t work hard enough.
Here’s the implication: strength and tolerance are not the same quality, and training one does not automatically produce the other.
Strength is the capacity to generate force. Tolerance is the capacity to absorb it. Both are necessary. Neither is sufficient alone.
A 2011 study by McGill and colleagues demonstrated that spinal stability—measured as resistance to buckling under applied load—was more dependent on the precise timing and coordination of muscular activation than on the absolute force-generating capacity of the muscles involved. A perfectly timed activation of a relatively weak deep stabilizer contributed more to segmental control than a powerful but delayed activation of a superficial global muscle.
This has direct clinical consequences. A rehabilitation program that trains only the global muscles—that prioritizes load and resistance over timing and coordination—will produce a patient who is stronger but not necessarily more tolerant. Their nervous system may still be generating the same dysregulated, delayed, reactive pattern it learned in response to injury. They’ve added horsepower to a vehicle with faulty suspension.
There is also a pain-system dimension to the armor trap. Patients who have developed central sensitization—as many post-collision patients have, often without knowing it—experience increased pain during movement not because their structure is failing but because their pain-detection system is set too sensitively. When these patients encounter pain during exercise, the natural response is to brace harder, move less, and protect more. This bracing increases compressive load on already sensitized structures, which generates more nociceptive input, which maintains the sensitization, which makes movement more painful.
The armor trap is a loop. Bracing generates the pain that justifies more bracing. And the tolerance system—which requires movement, load, and proprioceptive input to recover—atrophies further with each cycle of avoidance.
Breaking the armor trap requires understanding that the path to stability runs through tolerance, and tolerance is built by controlled, progressive, precisely monitored exposure to load—not by avoiding it.
Section 5: Graded Exposure — The Science of Rebuilding Tolerance
If tolerance is a system capacity—not a structural property but a dynamic, trainable quality—then the question becomes: how do you train it?
The answer, supported by a convergent body of research in pain science, sports medicine, and rehabilitation neuroscience, is graded exposure: the progressive, systematic introduction of load, movement, and perturbation in quantities and qualities that challenge the tolerance system without overwhelming it.
Graded exposure works through several overlapping mechanisms.
Restoring proprioceptive fidelity. Before the deep stabilizing system can function correctly, the neural control system needs accurate input. Proprioceptive training—joint repositioning tasks, balance challenges, sensorimotor exercises that require precise postural adjustment—restores the quality of afferent signaling from the injured region. As proprioceptive accuracy improves, the timing and coordination of deep stabilizer activation begins to normalize. This is not strength training; it is neural re-education.
Re-establishing feedforward activation. Research by Hodges, Jull, and their colleagues has demonstrated that specific low-load exercises targeting the deep stabilizers can restore feedforward timing when performed with appropriate precision and feedback. The cranio-cervical flexion test, for example, trains selective activation of the longus colli and longus capitis at low intensity, with real-time feedback to prevent superficial muscle substitution. The goal is not contraction magnitude but contraction quality and timing. Small, precise, correctly timed: these are the parameters that rebuild the anticipatory system the injury disrupted.
Progressive load tolerance. Once the deep system is re-engaging with appropriate timing, load can be progressively introduced. The principle here is drawn from the science of tissue loading: both muscles and connective tissues adapt their tolerance capacity in response to load—but only when that load is appropriately calibrated. Too little load produces no adaptation. Too much load produces re-injury or pain-system flare that sets back progress. The sweet spot—what researchers call the “anabolic window” for tissue adaptation—is load that is challenging but manageable, that produces some metabolic stress without triggering protective guarding or pain-system sensitization.
This calibration is clinical art as much as science. It requires monitoring not just objective markers—how much weight, how many repetitions—but subjective ones: the patient’s sense of control during the movement, their pain response in the 24 hours after exercise, their ability to maintain precise coordination under increasing demand. A patient who can perform a perfect deep neck flexor contraction at zero load but collapses into superficial compensation the moment a small resistance is added has not yet built enough tolerance for that load level.
Perturbation training. The final layer of tolerance training involves unpredictable, externally imposed challenges to balance and segmental control. Real life does not provide loads in controlled, predictable increments. A car stops suddenly. A foot lands on uneven ground. A colleague bumps your shoulder in a hallway. These events require the nervous system to generate a protective response faster than conscious control allows—exactly the feedforward and rapid reflex capacity that injury disrupts.
Perturbation training gradually re-exposes the nervous system to unpredictable demands in controlled clinical conditions, progressively rebuilding the reflex arcs and anticipatory patterns that allow the body to absorb the unexpected without losing control. Research on perturbation training for knee injury rehabilitation has demonstrated restoration of neuromuscular control, reduced re-injury rates, and improved functional outcomes compared to strength training alone. The same principles apply to the spine.
The timeline for this work is measured in weeks to months, not days. Tolerance is not a quick adaptation. Ligamentous healing proceeds on a collagen remodeling timeline of three to twelve months. Neurological re-patterning requires repetition sufficient to consolidate new motor programs. Tissue load tolerance increases incrementally with each training cycle. There is no shortcut—but the compound effect of correctly executed graded exposure is a body that can absorb what the world throws at it.
“Rehabilitation that never reintroduces unpredictability produces a patient who performs well in clinical settings and fails in life.”
The TimelineTolerance is not a quick adaptation. Ligamentous remodeling takes 3–12 months. Neurological re-patterning requires repetition sufficient to consolidate new motor programs. There is no shortcut—but the compound effect of correctly executed graded exposure is a body that absorbs what life throws at it.
Section 6: What This Means for Personal Injury Recovery
In the context of personal injury cases, the stability-as-tolerance framework has implications that extend beyond clinical care.
Insurance systems often evaluate injury severity and recovery trajectory through a structural lens: what was damaged, when did it heal, and is the patient now structurally intact? This framework misses the tolerance dimension entirely. A patient can be structurally healed—ligaments repaired, disc integrity restored, facet joints no longer acutely inflamed—while still having significantly impaired tolerance capacity.
Their deep stabilizing system may still be dysregulated. Their feedforward timing may still be delayed. Their proprioceptive fidelity may still be degraded. Their pain system may still be sensitized to loads that a pre-injury body would have absorbed without consequence.
These are measurable deficits. The cranio-cervical flexion test quantifies deep flexor function and endurance. Cervical joint position sense testing quantifies proprioceptive accuracy. Force plate analysis during perturbation challenges quantifies neuromuscular response timing. These are not subjective complaints—they are objective findings that document the gap between structural healing and functional tolerance.
And that gap matters enormously for the patient’s actual capacity to function—to work, to drive, to exercise, to perform the activities of daily life without pain, guarding, and the constant fear of re-injury.
A patient who reaches the structural healing milestone but has not yet restored their tolerance capacity is not recovered. They are simply waiting to be hurt again by forces that their pre-injury body would never have noticed.
This is why the duration and focus of appropriate post-injury rehabilitation extends well beyond the point at which structural healing is complete. The rebuilding of tolerance—proprioceptive re-education, deep stabilizer retraining, progressive load exposure, perturbation training—is the second phase of recovery, and it is the phase that determines whether the patient actually returns to full function or merely to the appearance of it.
In my experience, patients who complete both phases—structural recovery and tolerance restoration—return to their pre-injury lives with genuine confidence. They can move without bracing. They can absorb an unexpected load without flinching. They trust their bodies again.
Patients who receive only the first phase—or who are discharged from care when structural healing is deemed complete without addressing the tolerance deficit—often do not. They live in armor. Functional, perhaps. But guarded, limited, and waiting.
Conclusion: Strength Without Tolerance Is Just Armor
The thesis of this essay is both biomechanical and philosophical.
Biomechanically: stability is not rigidity. It is not the absence of movement or the presence of maximum compression. It is the nervous system’s capacity to coordinate muscles, process proprioceptive input, generate anticipatory responses, and modulate stiffness in real time—all in service of absorbing forces that cannot be predicted or controlled.
Philosophically: the goal of recovery is not to build a body that cannot be moved. It is to build a body that can be moved, loaded, perturbed, and surprised—and respond without failing.
Strength is part of that. But strength without tolerance is just armor. Heavy, brittle, exhausting to maintain, and ultimately unable to do what a living body actually needs to do: adapt to a world that will not always announce itself before it arrives.
The path from injury to genuine resilience runs through tolerance. Through restoring proprioceptive fidelity. Through rebuilding the deep stabilizing system’s timing and precision. Through progressive, well-calibrated exposure to load. Through re-educating the nervous system that movement is safe again.
This is not a quick path. But it is the correct one. And in twenty-five years of watching patients navigate it, I have seen what waits on the other side: a body that trusts itself again. A body that absorbs life’s forces without bracing against them.
Not armor. Tolerance. That is what stability actually is.
This article is for educational purposes. If you have been in a motor vehicle accident or suffered a musculoskeletal injury, consult a qualified healthcare provider for evaluation and treatment specific to your situation.
Adjust Clinic — Sonoma County Personal Injury Chiropractic
