But something did happen. Inside the vehicle, a human body absorbed a rapid transfer of kinetic energy. The cervical spine flexed and extended through a range of motion it was never designed to endure at that velocity. Ligaments stretched. Muscles tore at a microscopic level. Neural pathways fired distress signals that would take hours, sometimes days, to fully register.
"Where others see a fender bender, we must see a person who deserves understanding and care. Responsibility begins where dismissal ends."
This analysis draws on biomechanical research, clinical outcome studies, and neuropsychological evidence to make the case that low-speed collisions deserve the same clinical seriousness we afford to any mechanism of injury capable of producing lasting harm.
The Physics of "Minor": Why Less Damage Can Mean More Force
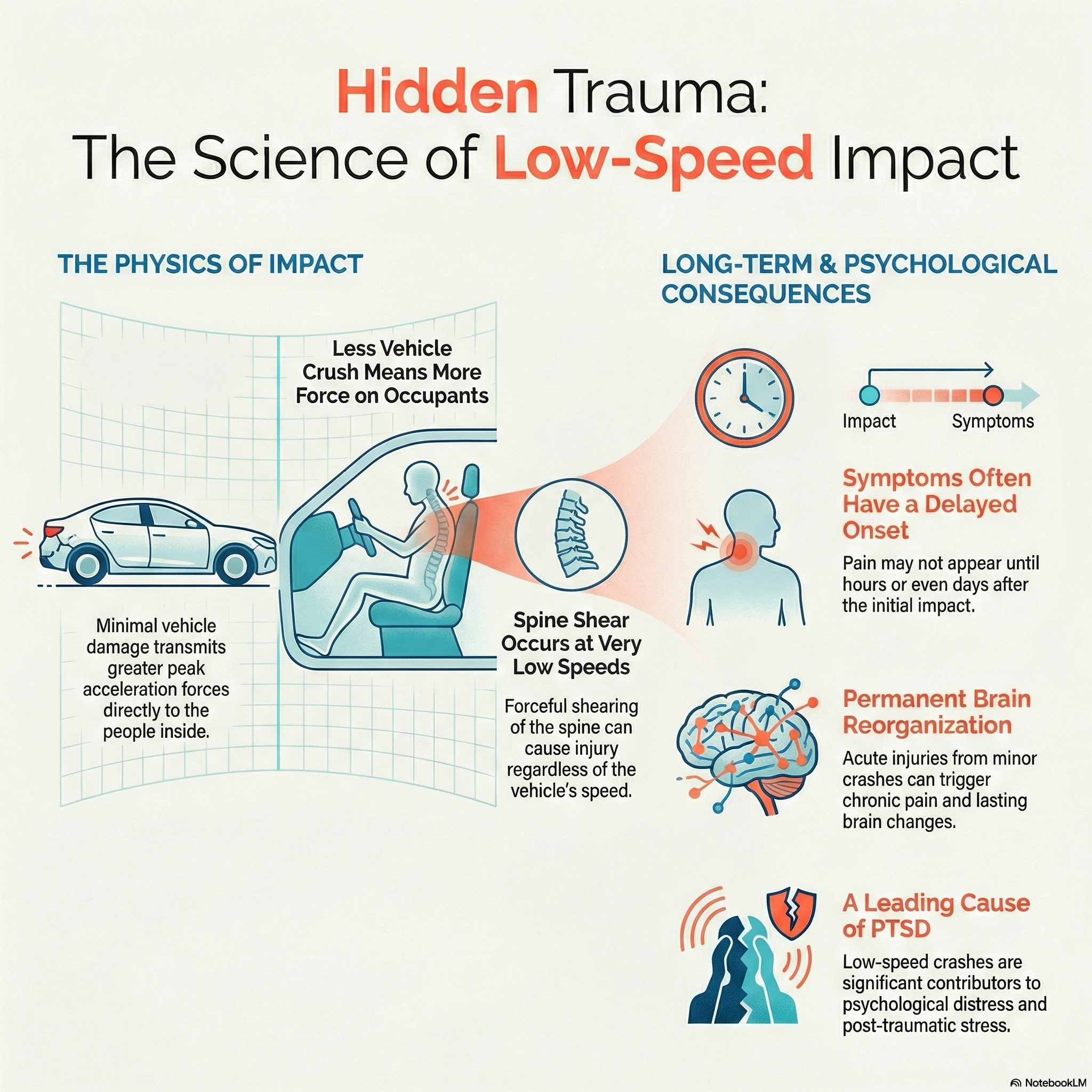
The single most persistent myth in motor vehicle injury assessment is the assumption that minimal vehicle damage equals minimal occupant injury. This belief is not only unsupported by physics — it is, in many scenarios, inverted.
Malcolm C. Robbins, an engineer with the Society of Automotive Engineers, stated plainly that "a common misconception formulated is that the amount of vehicle crash damage due to a collision offers direct correlation to the degree of the occupant injury." His work demonstrated that vehicles with very little crush distance can actually subject their occupants to greater accelerations, even at low indicated speeds.
The principle at work is conservation of energy. In any collision, kinetic energy must go somewhere. In higher-speed crashes, a large portion of that energy is absorbed by the deformation — the crumpling — of the vehicle's structure. That structural crush acts as a buffer, extending the duration of the impact and reducing the peak forces transmitted to the occupants.
⚠️ Critical Engineering Finding
The National Highway Traffic Safety Administration (NHTSA) mandates that vehicle bumpers sustain no damage at impacts up to 2.5 mph. This means the bumper bounces back — and the energy that would have been absorbed by metal deformation is instead transferred directly to the occupants inside the vehicle.
As J. Smith noted in his 1993 research: "The absence or presence of vehicle damage is not a reliable indicator of injury potential in rear impacts. Based upon the principle of conservation of energy, any energy which does not go into damaging the vehicle must be converted into kinetic energy, the source of injuries."
A 1997 Society of Automotive Engineers article provided a striking example: the same 25 mph collision resulted in five times greater force on occupants when the crush distance dropped from 1 meter to 0.2 meters. Less crush means a shorter stopping distance, which means higher peak acceleration — and that acceleration is what injures people.
The physics equation governing this is straightforward:
a = V² / 2s
Where a is acceleration, V is velocity of impact, and s is the crush distance.
As s approaches zero — as it does in a low-speed "no damage" collision — the acceleration experienced by the occupant rises sharply.
"A pristine bumper after a collision is not evidence that nothing happened. It may actually be evidence that more force was transmitted to the person inside."
The Biomechanics of Whiplash: What Happens Inside the Neck
The term "whiplash" has been trivialized by decades of cultural skepticism, but the underlying biomechanics are well documented and clinically significant.
During a rear-end collision, even at speeds as low as 5–10 mph, the occupant's torso is driven forward by the seat back while the head momentarily lags behind due to inertia. This creates a shearing force across the cervical spine — the head moves backward relative to the torso before being whipped forward. This all occurs within approximately 100–300 milliseconds, far too fast for any voluntary muscular response.
Research using crash dummies, cadavers, human volunteers, and computer models has confirmed that the cervical spine is subjected to a horizontal shear or retraction during the initial stages of rear-end collisions. These studies have identified multiple tissues vulnerable to damage during this event:
- Anterior longitudinal ligament — which can be stretched or partially torn
- Intervertebral discs — which can sustain annular tears
- Facet joint capsules — which may be strained beyond their physiological range
- Cervical musculature — which undergoes eccentric loading it cannot adequately resist
- Vertebral arteries — which may be transiently compressed or stretched
📊 Research Finding
Approximately 85% of neck injuries caused by car accidents are the result of rear-end collisions — the very collision type most likely to produce minimal vehicle damage.
Emori's research (1990) found that neck extension reaches nearly 60 degrees — a recognized danger threshold for whiplash — at collision speeds as low as 2.5 km/h (approximately 1.5 mph). McConnell et al. (1993) concluded that delta-V values of just 5 mph represent a probable threshold for cervical injury.
"There is no safe speed threshold below which cervical injury can be ruled out."
A 2018 study published in Patient Safety in Surgery examining real-world collision data found that cervical spine injuries occurred across a wide range of delta-V values in rear-end collisions, from as low as 9 km/h to 37 km/h. The researchers concluded that it was "impossible to define a ΔV value that excluded the occurrence of cervical spine injury with acceptable sensitivity while simultaneously predicting the occurrence of cervical spine injury with acceptable specificity." In plain terms: there is no safe speed threshold below which cervical injury can be ruled out.
Delayed Onset: The Biological Time Bomb
One of the most dangerous aspects of low-speed collision injuries is the delay between the event and the onset of symptoms. This delay feeds the cultural narrative that "it wasn't that bad" — and by the time symptoms fully emerge, the connection to the collision may be questioned by insurers, employers, and sometimes even clinicians.
⏰ Critical Timeline
According to the American Academy of Physical Medicine and Rehabilitation, up to two-thirds of people report neck pain within several hours of injury, while another third experience delayed onset of up to 48 hours.
Initial complaints often include neck and upper back pain, but a wider constellation of symptoms — headaches, dizziness, concentration difficulties, memory disturbances, upper limb paresthesias, and blurred vision — frequently accompanies or follows the initial presentation. These have been formally classified as Whiplash-Associated Disorders (WAD).
Radanov et al. reported that the delay in headache onset averaged 10 hours and neck pain onset averaged 11 hours in patients who eventually recovered. In patients who did not recover within two years, the delays were shorter — 4 and 8 hours respectively — but the variation ranged from minutes to days. The researchers noted that these symptom delays "favour a slowly evolving pathology rather than an immediate sprain lesion," suggesting that the injury process unfolds over time at the cellular and tissue level.
This slow evolution makes biological sense. In the hours following mechanical trauma, inflammatory cascades activate. Damaged tissues swell. Micro-hemorrhages develop in muscle and ligamentous tissue. Neural sensitization begins. The adrenaline and cortisol surge that accompanies any traumatic event masks pain signals initially, and as these stress hormones subside, the true extent of tissue disruption reveals itself.
"The absence of immediate symptoms does not rule out significant injury."
For clinicians, this has an important implication: the absence of immediate symptoms does not rule out significant injury. For patients, the cultural pressure to "shake it off" after a minor-looking crash can lead them to delay treatment during the very window when early intervention matters most.
The Chronic Pain Trajectory: From Weeks to Years
Perhaps the most consequential finding in whiplash research is the rate at which acute injuries transition to chronic conditions.
The AAPM&R reports that while approximately 50% of whiplash symptoms resolve within 1–2 weeks, and 90% resolve within 6–12 weeks, the patients who do not recover face a distinctly challenging trajectory. Once pain persists beyond 3 months and enters the chronic phase, it becomes significantly more difficult to treat. Among patients with persistent symptoms, approximately 85% experience symptom recurrence within 1–2 years.
📈 Long-Term Outcomes
Research estimates that between 14% and 42% of people who sustain whiplash develop chronic symptoms, with the percentage varying between 2% and 58% across different studies, with symptoms persisting for years in many cases.
A landmark study from Northwestern University, published in Nature Mental Health in October 2024, shed light on why some people develop chronic pain after injury while others recover. Researchers found that within just three days of an injury, the brain can adapt in ways that predict chronic pain development. Specifically, the more the hippocampus (the brain's memory center) communicated with the cortex (involved in long-term memory storage), the more likely the person was to develop chronic pain. High anxiety levels immediately following the accident further strengthened this prediction.
This is a critical finding. It means the transition from acute to chronic pain is not simply a matter of tissue healing or failure to heal — it involves central nervous system reorganization that begins almost immediately after injury. Early intervention, therefore, is not just about treating the local tissue damage but about interrupting a neurological cascade that can cement pain into the patient's long-term experience.
The downstream effects of chronic pain are well documented: muscle weakness from disuse, compensatory movement patterns that strain other joints and tissues, degenerative disc changes, sleep disruption, fatigue, and a progressive erosion of functional capacity that affects everything from work performance to personal relationships.
The Psychological Wound: PTSD, Anxiety, and Depression
The injuries that follow a low-speed collision are not confined to the musculoskeletal system. The psychological impact of motor vehicle collisions is substantial, well-documented, and frequently overlooked.
🧠 Mental Health Impact
Motor vehicle accidents are the leading cause of post-traumatic stress disorder (PTSD) in the general civilian population in the United States, affecting an estimated 2.5 to 7 million people. PTSD affects approximately 32.3% of car accident survivors, with some studies reporting rates as high as 45%.
A study published in the American Journal of Psychiatry found that at least one-third of consecutive patients presenting to an emergency department following a motor vehicle accident developed persistent psychiatric disorders — even among those with "medically minor" physical injuries. The researchers concluded that those at high risk of chronic psychological difficulties could be recognized clinically soon after the accident and offered early treatment.
Post-traumatic stress symptoms (PTSS) and sensory hypersensitivity are now recognized as established predictors of poor outcome after whiplash injury. A 2022 cohort study of 740 patients found that those with clinical PTSS exhibited sensory hypersensitivity across all time points over 12 months, along with greater pain intensity and more widespread pain distribution — demonstrating a clear and measurable link between psychological trauma and physical outcomes.
The psychological fallout extends beyond PTSD:
- Anxiety disorders — including driving phobias and generalized anxiety — are common and can persist for months to years
- Depression — with one study finding that 21.3% of collision survivors met clinically relevant thresholds for depression
- Sleep disturbances — insomnia and disrupted sleep architecture compound both psychological and physical recovery
- Acute stress reactions — intrusive memories, hypervigilance, and avoidance behaviors that may not meet full PTSD criteria but significantly impair quality of life
Importantly, poor psychological health directly impedes physical healing. Chronic stress weakens immune function, increases systemic inflammation, and disrupts the neurobiological processes necessary for tissue repair. The mind and body are not separate recovery tracks — they are the same track.
The Vulnerability Gap: Who Gets Hurt Most
Not all bodies respond equally to the same collision forces, and this variability is another reason vehicle damage is a poor proxy for human injury.
⚖️ Gender Disparity
Women are 1.5 to 4 times more likely to develop chronic pain from whiplash than men. Females show a consistently higher risk of whiplash injury across age groups, collision types, and seating positions.
The reasons are multifactorial — differences in neck musculature, cervical spine geometry, hormonal influences on connective tissue, and varying pain processing pathways all contribute.
Age plays a significant role. Older adults often experience longer-lasting symptoms, while pre-existing degenerative changes in the cervical spine — common even in asymptomatic individuals over 40 — create a vulnerability that a low-speed collision can exploit. A disc that was silently narrowing for a decade may herniate under forces that a younger spine would tolerate.
Pre-existing conditions — prior neck injuries, headache disorders, anxiety, depression, and chronic pain syndromes — all lower the threshold at which a collision produces lasting symptoms. The legal doctrine of the "eggshell plaintiff" exists precisely because the law recognizes what medicine confirms: you take the patient as you find them.
Head position at the moment of impact matters enormously. A head turned even slightly to one side alters the biomechanical loading on the cervical spine, potentially concentrating forces on one facet joint or stretching one vertebral artery disproportionately. A person checking their mirror, reaching for something, or turning to speak to a passenger is at materially greater risk than someone facing straight ahead.
Awareness of the impending collision also influences outcomes. Occupants who brace before impact activate cervical musculature that provides some protective stiffening. Those who are struck without warning — the vast majority of rear-end collision victims — have no muscular defense against the initial shear forces.
These variables mean that two people in the identical collision can have dramatically different outcomes. This is not evidence that one person is exaggerating — it is evidence that human beings are not standardized crash test dummies.
The Cultural Problem: Dismissal as Default
There is a powerful cultural machinery that minimizes low-speed collision injuries. It operates at every level:
Insurance industry practices. The strategy of correlating vehicle damage with injury severity is not a neutral scientific assessment — it is a claims management tool. "Low impact" or "minor impact soft tissue" (MIST) programs were explicitly designed to reduce payouts on claims arising from collisions with minimal property damage, regardless of the occupant's actual clinical presentation.
Emergency department triage. In busy emergency rooms, a patient who walks in after a low-speed collision, with normal neurological findings and unremarkable imaging, may be told they have a "sprain" or "strain," given ibuprofen, and sent home. There is often no discussion of the natural history of whiplash, no warning about delayed symptom onset, no recommendation for follow-up care, and no screening for psychological distress.
Social minimization. Friends, family, coworkers, and even other healthcare providers may express skepticism: "It was just a fender bender." "You look fine." "My cousin had a worse accident and was fine in a week." This informal dismissal compounds the patient's doubt about their own experience and can delay help-seeking.
Self-dismissal. Patients themselves internalize these messages. Adrenaline masks early symptoms. Cultural pressure to be "tough" discourages complaint. The visual evidence — a car that looks fine — conflicts with the internal evidence of pain and dysfunction. Many patients talk themselves out of seeking care, only to present weeks or months later with entrenched symptoms that are now harder to treat.
This cycle of dismissal has real consequences. Delayed treatment is consistently associated with poorer outcomes. Early intervention — whether chiropractic, physical therapy, or psychological support — interrupts the progression from acute injury to chronic condition. Every day of dismissal is a day the inflammatory cascade advances, the neural sensitization deepens, and the window for optimal recovery narrows.
What the Evidence Demands of Clinicians
The research literature points to several clear imperatives for clinicians who encounter patients after low-speed collisions:
- Take the mechanism seriously, regardless of vehicle damage. The absence of vehicle deformation may actually indicate greater force transmission to the occupant. Clinical assessment should be driven by patient presentation, not by property damage photos.
- Educate patients about delayed symptom onset. Patients should be informed that symptoms may emerge or intensify over 24–72 hours, and that this does not mean the injury is "in their head" — it means the inflammatory and neurological response is unfolding on its own timeline.
- Screen for psychological distress early. Given that PTSD symptoms and high anxiety are established predictors of poor recovery, brief screening tools should be part of the initial evaluation. Early identification allows for early referral and intervention.
- Document thoroughly. Comprehensive documentation of the mechanism of injury, the patient's immediate and evolving symptoms, and their functional limitations is not just good medicine — it is the patient's defense against the dismissal they will inevitably face from insurers and, sometimes, other providers.
- Intervene early and consistently. The evidence supports early mobilization, manual therapy, graduated exercise, and psychological support. Passive waiting — "let's see if it gets better on its own" — is not supported by the evidence when the clinical presentation suggests WAD Grade II or higher.
- Account for individual vulnerability. Sex, age, pre-existing conditions, head position, and awareness at the time of impact all modify injury risk. A thorough history that captures these variables allows for more accurate prognosis and more appropriate treatment planning.
What the Evidence Demands of Society
Beyond the clinical encounter, the evidence calls for broader changes in how we think and talk about low-speed collisions:
Insurance practices must evolve. The use of vehicle damage as a proxy for injury severity is scientifically indefensible. Claims evaluation should incorporate clinical findings, patient-reported outcomes, and an understanding of the biomechanical principles that explain why minimal damage can coexist with significant injury.
Legal frameworks must protect patients. Injured individuals should not have to prove that their car was sufficiently damaged before their pain is taken seriously. Expert biomechanical testimony and updated judicial education can help bridge the gap between what the science says and what the courtroom assumes.
Public education matters. Most people do not know that a stiff bumper transfers more energy to occupants, that symptoms can be delayed by days, or that whiplash can become a chronic condition. Simple, evidence-based public health messaging could reduce delayed care-seeking and improve outcomes.
Language matters. The terms we use shape perception. Calling a collision "minor" because the cars look fine is a judgment about property, not people. Calling an injury "just whiplash" minimizes a condition that European insurance systems value at 10 to 20 billion euros annually in direct costs. The language of dismissal is the first barrier to appropriate care.
Conclusion: Responsibility Begins Where Dismissal Ends
The evidence is clear and it is not new. For over three decades, biomechanical engineers, clinicians, and researchers have documented that low-speed collisions can produce significant, lasting injuries — and that the extent of vehicle damage is an unreliable indicator of what happened to the person inside.
The physics explains why: less vehicle deformation means more energy transferred to the occupant. The biomechanics explains how: the cervical spine is subjected to shear forces that exceed tissue tolerance at remarkably low speeds. The clinical evidence explains what happens next: a substantial minority of patients develop chronic pain, psychological distress, and functional limitations that reshape their daily lives.
Every link in this chain is supported by peer-reviewed research. And yet, the dominant cultural response to a low-speed collision remains dismissal.
This is a failure of translation — a failure to bring what we know in the laboratory and the clinic into the adjustor's office, the courtroom, the emergency department waiting room, and the dinner table where a patient hears, "But your car looks fine."
"Where others see a fender bender, we must see a person. The question is not whether the car was damaged. The question is whether the person was damaged."
Where others see a fender bender, we must see a person. A person whose tissues have been stressed beyond their tolerance. A person whose nervous system may already be reorganizing toward chronic pain. A person who may be developing anxiety or PTSD that will affect every car ride for years to come. A person who deserves not skepticism, but clinical rigor. Not dismissal, but understanding.
Responsibility — clinical, institutional, and societal — begins exactly where dismissal ends. The question is not whether the car was damaged. The question is whether the person was damaged. And the only way to answer that question is to look at the person, listen to the person, and take what they are telling you seriously.
That is not soft medicine. That is evidence-based care.
