When the Bumper Holds, the Spine Pays
Direction and history matter more than speed — an evidence-based analysis of rear-end collision injuries, spinal biomechanics, and individual vulnerability.
Rear-end motor vehicle collisions are the single most common crash configuration on roads worldwide. They are also, by a wide margin, the most injurious to the human spine. This paradox — that the so-called “fender-bender” produces more neck and back pain claims than many high-speed collisions — has confounded insurers, attorneys, and even some clinicians for decades. The explanation lies not in velocity alone, but in physics, anatomy, and individual vulnerability.
Every year, millions of rear-end crashes occur at speeds that leave bumpers intact and paint barely scuffed. Yet these collisions fill chiropractic offices, orthopedic clinics, and courtrooms with patients reporting persistent neck pain, headaches, low back dysfunction, and radiating arm symptoms. The disconnect between vehicle damage and human injury is not a mystery. It is a well-documented biomechanical reality.

The forces generated in a rear-end impact follow a specific path through the human body. They enter through the seat back, accelerate the torso forward, and leave the head momentarily behind — creating a shearing force across the cervical spine that can exceed the tolerance of ligaments, joint capsules, and intervertebral discs. These forces do not travel through a blank slate. They travel through a spine shaped by decades of posture, prior injuries, degenerative changes, and muscular conditioning. Two occupants in the same vehicle, struck by the same force, can walk away with profoundly different outcomes.
The thesis of this analysis is direct: the severity of spinal injury after a rear-end collision depends less on how fast the vehicles were traveling and more on the direction of force, the timing of the occupant’s response, and the structural condition of the spine at the moment of impact. Understanding a patient’s history is not supplemental to understanding the crash. It is equally important.
The Epidemiology: A Disproportionate Threat
Rear-end collisions account for approximately 29 percent of all motor vehicle crashes in the United States, yet they produce a disproportionate share of soft-tissue spinal injuries. The National Highway Traffic Safety Administration (NHTSA) has consistently identified rear impacts as the leading cause of whiplash-associated disorders (WAD).
85–90%
of whiplash injuries originate from rear-end collisions — making them the single leading cause of whiplash-associated disorders.
The numbers for low back pain are equally striking. A forensic analysis of 83 cases involving low-velocity motor vehicle collisions found that 77 percent involved a claim of low back pain, and of those, 70 percent involved a rear-end collision configuration. Forty percent of all cases occurred at impact severities between just 10 and 12 km/h — speeds that most people would dismiss as trivial. The most common pre-existing medical condition among claimants was prior low back pain or evidence of disc degeneration.
2.7×
The relative risk of future low back pain after injury in a motor vehicle crash. 63% of ongoing low back pain can be attributed to the prior crash-related injury.
A systematic review and meta-analysis published in Accident Analysis & Prevention confirmed these figures. Importantly, the study also found that rear-end crashes without injury did not increase the risk of future low back pain — suggesting that the injury event itself, not merely the psychological experience of collision, drives the long-term pain trajectory.
Whiplash-associated disorders alone cost European insurance systems between 10 and 20 billion Deutsche Marks annually by the late 1990s. In the United States, whiplash accounts for an estimated $30 billion per year in economic costs including medical care, disability, and lost productivity. These are not fringe claims. They represent a public health problem of enormous scale, and the majority originate from impacts that cause little or no structural vehicle damage.
Delta-V and the Low-Speed Paradox
The single most misunderstood concept in crash-injury analysis is the relationship between vehicle speed and occupant injury. The relevant metric is not the speed of either vehicle, but delta-V — the change in velocity experienced by the struck vehicle during impact. Delta-V captures the magnitude of the acceleration pulse transmitted to the occupant, and it is the primary physical quantity correlated with injury risk.
But even delta-V tells only part of the story. The duration and shape of the acceleration pulse matter enormously. A sharp, short-duration pulse can produce far greater peak forces on spinal structures than a longer, more gradual one at the same delta-V. This is why a 15 km/h rear-end impact into a stationary vehicle can produce more cervical spine loading than a 30 km/h impact into a vehicle that is already rolling forward — the deceleration is abrupt in the first case and dampened in the second.
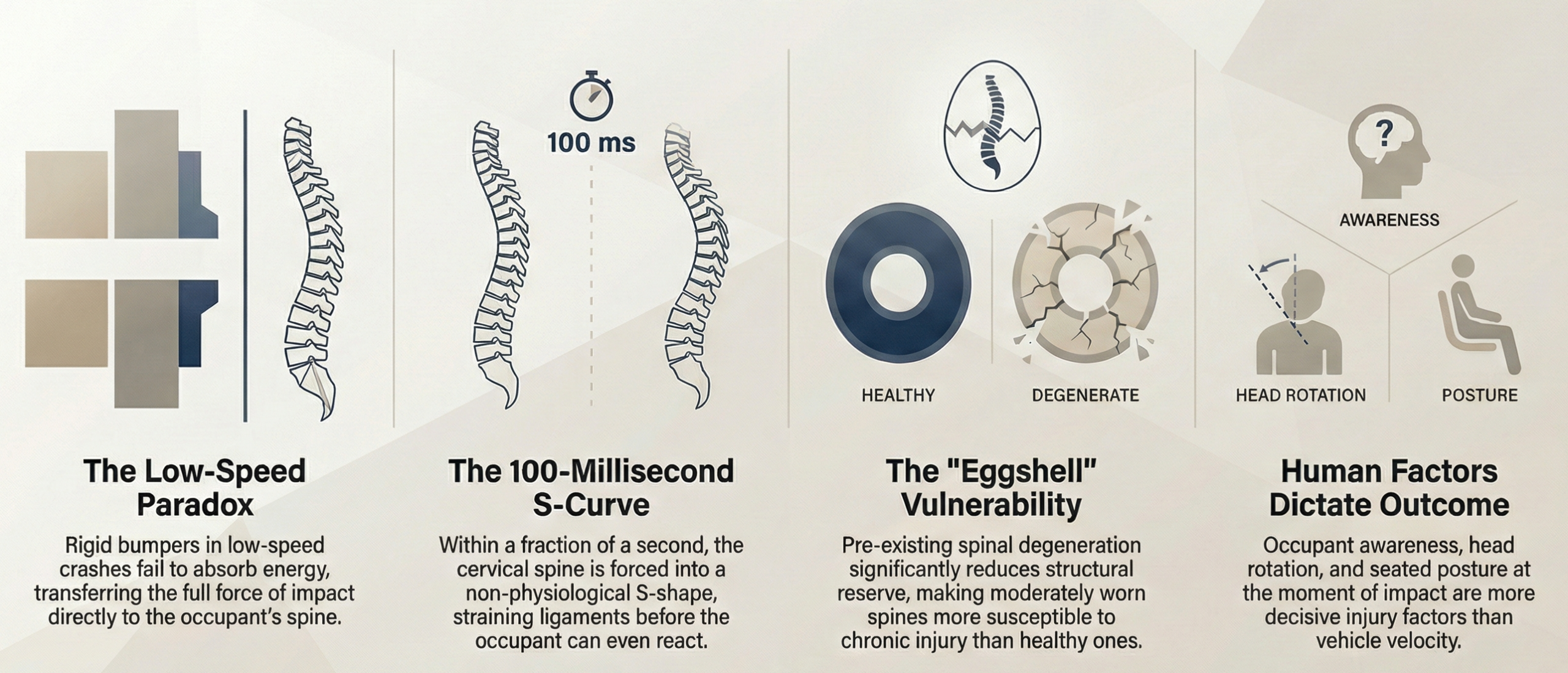
Here is where the low-speed paradox becomes critical. In low-speed rear-end collisions, the vehicle’s bumper and crush zones often do not deform significantly. Modern vehicles are engineered to resist damage at low speeds to reduce insurance repair costs. But when the vehicle structure remains rigid, it does not absorb kinetic energy through deformation. Instead, that energy is transferred more efficiently to the occupant.
“The vehicle that looks undamaged may have subjected its occupant to a more efficient energy transfer than a vehicle with visible bumper crush.”
Volunteer studies have documented this phenomenon repeatedly. A comprehensive review of all prior low-speed rear impact volunteer studies, published in the Journal of Forensic and Legal Medicine (2018), compared experimental data with real-world crash outcomes from the National Automotive Sampling System. The study found that injury symptoms occurred in real-world crashes at delta-V levels comparable to or only slightly above the thresholds tested in volunteer experiments — typically in the range of 4 to 8 km/h for symptom onset.
There is no scientifically established delta-V threshold below which whiplash injury cannot occur.
Claims that a crash was “too minor” to cause injury based on vehicle damage alone have no basis in the biomechanical literature.
Inside the Neck: The Biomechanics of Whiplash
The term “whiplash” is a misnomer in one important respect. The cervical spine does not move like a whip. It moves in a far more complex and damaging pattern.
During a rear-end impact, the seat back pushes the torso forward while the head, unsupported by inertia, lags behind. In the first 50 to 100 milliseconds — before the occupant is consciously aware that a collision has occurred — the cervical spine forms a transient S-shaped curve. The lower cervical vertebrae (C5–C7) are thrust into extension while the upper cervical vertebrae (C0–C2) are simultaneously pushed into relative flexion. This S-curve is not a normal physiological motion. It places the lower cervical facet joints, joint capsules, and intervertebral discs under abnormal compressive and shearing loads.

Research on cadaveric and finite-element models has shown that the facet joint capsular ligaments are the structures most vulnerable to strain during this S-curve phase. The capsular ligaments contain nociceptive nerve fibers, and sub-failure strains — stretching that damages tissue without completely tearing it — can trigger persistent pain signaling. This explains why many whiplash patients report pain that is real and measurable even when MRI and X-ray studies appear normal.
20–25%
of whiplash patients show cervical disc injury, with the C5–C6 level the most commonly affected segment.
After the initial S-curve, the head extends rearward until it contacts the head restraint (if one is present and properly positioned), then rebounds into flexion as the body decelerates. This secondary flexion phase places anterior cervical structures — the anterior longitudinal ligament, the disc annulus, and the longus colli muscles — under tensile load. The complete injury pattern is not extension or flexion, but a combined extension-flexion sequence with an injurious S-phase that occurs in the first fraction of a second.
Female occupants sustain whiplash at significantly higher rates than males, even in comparable crash conditions. Stemper and Corner (2016) attributed this in part to differences in neck morphology — smaller vertebral dimensions, lower cervical muscle mass, and greater range of cervical motion — that reduce the neck’s ability to resist the inertial loading of the head during impact.
65%
greater effectiveness of automotive whiplash-reduction safety features for males compared to females — underscoring how profoundly occupant anatomy shapes injury outcomes.
The Overlooked Injury: Low Back Pain in Rear-End Impacts
Conventional wisdom holds that the seat back “protects” the lumbar spine in a rear-end collision. This intuitive reasoning, while popular, is not supported by the evidence.
During a rear-end impact, the occupant’s pelvis is driven forward and upward along the angled seat back in a motion called ramping. This upward sliding compresses the lumbar spine axially while simultaneously changing its lordotic curve. The rapid forward acceleration of the pelvis relative to the upper body can load the lumbar facet joints, stretch the posterior lumbar ligaments, and increase intradiscal pressure — particularly at the L4–L5 and L5–S1 levels.
In some cases, the pelvis slides beneath the lap belt in a motion called submarining, which further increases axial loading on the lumbar spine and can concentrate shearing forces at the lumbosacral junction.
50%
of individuals in low-velocity rear-end collisions report low back pain. Approximately 25% develop chronic back pain that significantly affects daily activities.
The population-based Saskatchewan cohort study of 4,473 low back pain injury claims documented that low back pain is a common and often persistent consequence of rear-end crashes, with recovery timelines varying based on pre-existing conditions and psychosocial factors.
The 2020 systematic review confirmed the dose-response relationship: crash-related injury, not merely crash exposure, drives the risk of chronic low back pain. The tissue injury sustained at the time of collision — not the stress of the experience — is the primary pathological event. Treatment must therefore address the structural and functional consequences of that injury.
The Spine You Bring to the Crash
Perhaps no factor is more consequential — and more frequently underestimated — than the condition of the spine before the collision occurs. The same force that causes a transient ache in a healthy 25-year-old can trigger a disabling pain syndrome in a 55-year-old with multilevel facet arthropathy and disc desiccation. This is not speculation. It is the consistent finding of the best available research.

A landmark study published in the International Journal of Spine Surgery (2021) found a significant association between moderate facet joint degeneration and non-recovery after whiplash trauma — directly contradicting the prevailing clinical dogma that pre-existing degeneration does not affect whiplash outcomes.
The mechanism is logical. Degenerative changes in the facet joints lead to thinning of articular cartilage and hypermobility of the affected spinal segments. This hypermobility increases laxity of the facet joint capsule. When the capsule is subjected to the abnormal tensile stress of a whiplash mechanism, the collagen fibers are more likely to rupture. These ruptured fibers heal with scar tissue that lacks the mechanical properties of normal collagen — creating a joint that is both structurally weaker and more pain-sensitive than it was before the collision.
“The spine that is moderately worn is more vulnerable than the spine that is either pristine or fully fused.”
In advanced degeneration, the vertebral bodies may undergo ankylosis — bony fusion — that paradoxically increases segmental stability. Disc degeneration compounds the risk through a different pathway: desiccated discs lose height, narrowing the neural foramina and spinal canal. Studies have identified pre-existing canal narrowing at C5–C6 as a risk factor for low-grade spinal cord injury during whiplash.
Prior low back pain and prior disc degeneration were the most common pre-existing conditions identified in the forensic analysis of low-velocity crash claims. Patients starting from a position of reduced structural reserve face a narrower margin between tolerable loading and tissue failure.
The legal principle is well established: the “eggshell plaintiff” doctrine holds that a defendant takes the plaintiff as they find them. The biomechanical evidence now provides a robust scientific foundation for this legal principle.
Vector, Timing, and Awareness: The Real Determinants of Injury
If speed were the dominant variable in collision injury, frontal impacts at highway speeds would produce more whiplash than low-speed rear-end impacts. They do not. The direction of force — the vector — is the critical variable, and rear-end impacts are biomechanically unique in their capacity to injure the cervical spine.
In a frontal collision, the occupant is decelerated by the seatbelt and airbag, which distribute forces across the chest and limit cervical spine excursion. In a rear-end collision, there is no comparable restraint. The differential acceleration between torso and head is what creates the injurious S-curve. No other crash vector produces this specific loading pattern with the same efficiency.
Oblique rear impacts add a rotational component that further increases injury risk. If the occupant’s head is turned at the moment of impact, the cervical facet joints on the side of rotation experience concentrated loads that can exceed capsular failure thresholds at lower overall delta-V values.
Occupant awareness dramatically modifies injury risk. Kumar, Narayan, and Amell (2000) demonstrated that awareness of an impending impact significantly reduced head-neck accelerations. When occupants braced, muscles provided dynamic stabilization. In real-world rear-end crashes, the vast majority of victims are unaware of the impending impact.
“Comparing whiplash injuries to amusement park bumper car impacts is fundamentally misleading. Bumper car occupants are aware, braced, and anticipating contact. The occupant stopped at a red light who is struck from behind has none of these protective advantages.”
Seated posture adds another layer. If the occupant is leaning forward, the head restraint gap widens — consistently identified as one of the strongest predictors of whiplash injury severity. Two occupants in the same vehicle, subjected to the same delta-V, can experience vastly different outcomes. Velocity is one variable among many, and rarely the most important one.
Clinical Implications: History as Diagnosis
“The crash report tells you what happened to the vehicle. The patient’s history tells you what happened to the spine.”

A thorough clinical evaluation after a rear-end collision should include:
Pre-collision spinal history. Has the patient experienced prior neck or back pain? Prior motor vehicle collisions? Occupational loading? Degenerative changes on prior imaging? Each of these factors modifies the spine’s structural reserve and changes the injury threshold.
Occupant position and awareness at the time of impact. Was the patient aware of the impending collision? Were they braced or relaxed? Was the head turned? Were they leaning forward?
Head restraint and seat geometry. Was the head restraint properly positioned? Many head restraints sit too low — behind the neck rather than behind the head — offering no meaningful protection.
Symptom onset and evolution. Delayed symptom onset is characteristic of soft tissue and capsular injuries and should not be interpreted as evidence against injury causation. Many patients feel “fine” at the scene only to develop significant symptoms within 24 to 72 hours.
Imaging interpretation in context. Degenerative findings on post-collision imaging are frequently dismissed as “age-related.” The evidence suggests this dismissal is premature. The degeneration and the trauma interact — they cannot be cleanly separated.
The clinician’s role is to construct a biomechanical narrative that connects the mechanism of injury to the patient’s pre-existing anatomy and to the clinical findings. This narrative is the foundation of accurate diagnosis, appropriate treatment planning, and compelling medicolegal documentation.
Velocity Is Not Destiny
The evidence is unambiguous. Rear-end collisions produce a unique biomechanical insult to the human spine — one that operates through specific, well-characterized mechanisms that do not require high speed. Whiplash and low back injuries occur routinely at collision speeds below 25 km/h, at delta-V values that leave vehicles cosmetically intact.
Pre-existing degeneration does not protect the spine. In most cases, it sensitizes it. Moderate facet arthropathy, disc desiccation, and prior soft tissue injury all reduce the margin between tolerable and injurious loading. The “eggshell plaintiff” is not a legal fiction — it is a biomechanical reality confirmed by validated research.
“Understanding the patient who was in the crash is as important as understanding the crash itself.”
A thorough history, a detailed mechanism analysis, and an honest accounting of pre-existing vulnerability are not merely good clinical practice. They are the foundation of accurate diagnosis and effective advocacy for the injured patient.
References and Key Sources
- Cassidy JD et al. “Low back pain after traffic collisions: a population-based cohort study.” Spine 28(10), 2003.
- Croft AC. “Low Back Injuries in Low Velocity Rear Impact Collisions.” Consumer Attorneys of California FORUM, Jul/Aug 2009.
- Kumar S, Narayan Y, Amell T. “Role of awareness in head-neck acceleration in low velocity rear-end impacts.” Accident Analysis & Prevention 32(2), 2000.
- Pang D, Ritenour S. “Exposure to a motor vehicle collision and the risk of future back pain: A systematic review and meta-analysis.” Accident Analysis & Prevention 141, 2020.
- Rydman E et al. “Association between cervical degeneration and self-perceived nonrecovery after whiplash injury.” The Spine Journal 20(6), 2020.
- Sagar S et al. “Is Preexisting Cervical Degeneration a Risk Factor for Poor Prognosis in Whiplash-Associated Disorder?” Int J Spine Surgery 15(4), 2021.
- Smith AC et al. “Potential associations between chronic whiplash and incomplete spinal cord injury.” Spinal Cord Series and Cases 1, 2015.
- Stemper BD, Corner BD. “Whiplash-Associated Disorders: Occupant Kinematics and Neck Morphology.” JOSPT 46(10), 2016.
- Sturzenegger M et al. “A Comprehensive Review of Low-Speed Rear Impact Volunteer Studies.” J Forensic and Legal Medicine 58, 2018.
- Yoganandan N et al. “Characterization of Acute and Chronic Whiplash-Associated Disorders.” JOSPT 39(5), 2009.
