Sarah reached behind her back, trying to knead out the burning knot between her shoulder blades. "It's killing me right here," she told me during her initial exam, pressing her fingers into the spot just medial to her scapula. "But when I turn my head... that's when it really flares up."
I see this pattern weekly in our Petaluma clinic. Patients come in convinced their problem is in their shoulder blade—that's where it hurts, after all. But when we examine their neck, we find the actual culprit: a facet joint irritation at C5-6, or a trigger point in the levator scapulae, sending pain signals down a well-worn neural pathway to a spot that feels miles away from the source.
This phenomenon—pain felt in one area while originating from another—is called referred pain. And when it comes to neck problems manifesting as shoulder blade pain, it's one of the most common patterns we see after motor vehicle accidents.
The Highway System of Pain: How Referred Pain Actually Works
Your nervous system is like a vast highway network, with sensory information traveling from your tissues to your brain. But unlike a GPS with perfect routing, this system has some quirks—specifically, convergence points where multiple "roads" merge.
Here's what happens at the spinal cord level:
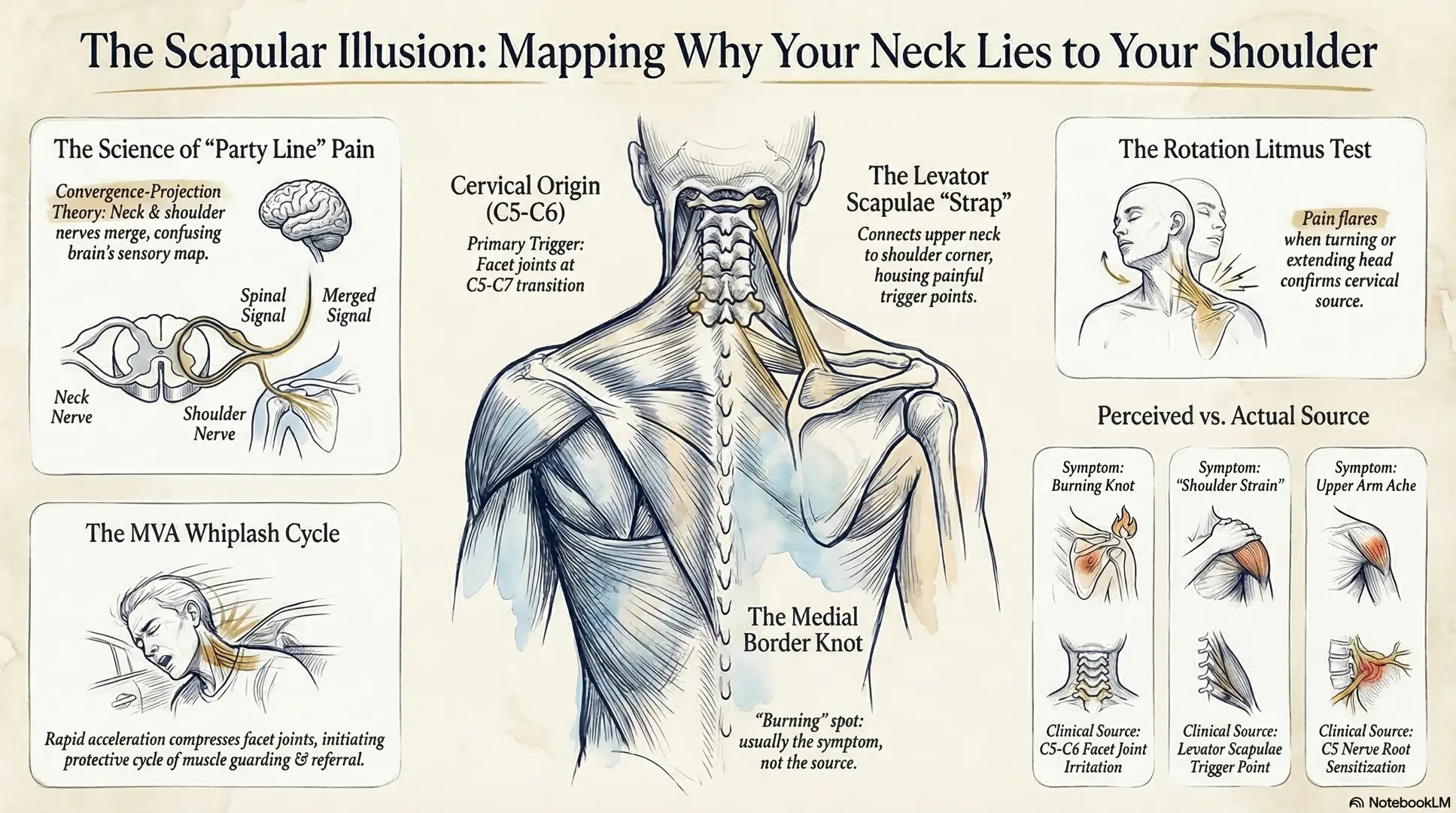
When nerve fibers from your neck muscles, facet joints, and discs enter the spinal cord, they converge with nerve fibers from your shoulder blade region in the same segment of the dorsal horn (the sensory processing center of your spinal cord). Your brain receives this mixed signal and sometimes can't tell which tissue the pain is actually coming from—so it "refers" the sensation to the more superficial, commonly injured area: your shoulder blade.[1]
Think of it like old telephone party lines where multiple households shared the same wire. Your brain is listening to the line, but it can't always tell which house is making the call.
The Dermatomal Connection
Each spinal nerve supplies sensation to a specific region of skin called a dermatome. The C5 nerve root, for example, covers the outer shoulder and upper arm. But here's the catch: that same nerve segment also receives deep pain signals from cervical facet joints, intervertebral discs, and the muscles that stabilize your neck.[2]
When a C5-6 facet joint gets irritated—say, from whiplash mechanics in a rear-end collision—your brain may interpret that deep, achy pain as coming from the C5 dermatome at the top of your shoulder blade, even though the actual problem is in your neck.
Why Motor Vehicle Accidents Create This Pattern
After a car accident, especially rear-impact collisions, your cervical spine experiences rapid acceleration-deceleration forces. Research shows this creates:
1. Facet Joint Irritation
The small joints that guide movement between your vertebrae (facet joints) get compressed and inflamed. The C5-6 and C6-7 facet joints are particularly vulnerable because they sit at the transition point where your mobile neck meets your more stable mid-back.[3] These joints are richly innervated with pain-sensitive nerve endings, and when irritated, they commonly refer pain to the medial border of your shoulder blade.
2. Muscle Guarding and Trigger Points
Your body's protective response creates sustained muscle tension. The levator scapulae—a strap-like muscle running from your upper cervical vertebrae to the top corner of your shoulder blade—often develops trigger points (hyperirritable spots in tight muscle bands) that refer pain in predictable patterns down to the scapular region.[4]
In Sarah's case, her levator scapulae was rock-hard on palpation, and when I pressed on the trigger point near her C3-4 vertebrae, she said, "That's it! That's the exact spot in my shoulder blade!"
3. Nerve Root Sensitization
Sometimes disc injuries or facet inflammation irritate the nerve root itself without causing frank compression. This creates what we call peripheral sensitization—the nerve becomes hyperexcitable and amplifies pain signals throughout its entire distribution.[5] You might feel pain anywhere along that nerve's pathway, not just at the injury site.
The Clinical Picture: What We See in Practice
When a patient presents with interscapular (between the shoulder blades) pain after an MVA, we look for these telltale signs of cervical origin:
Pattern Recognition:
- Pain that worsens with neck movements, especially rotation or extension
- Morning stiffness in both the neck and shoulder blade region
- Pain that changes position when you change your head position
- Relief when you support your head with your hand
On Examination:
- Restricted cervical range of motion (you can't turn your head as far as you should)
- Tenderness over specific cervical segments when we palpate (press on) your neck
- Positive Spurling's test (neck extension with rotation reproduces the shoulder blade pain)
- Tight, ropey bands in the cervical paraspinal muscles with palpable trigger points
Sarah demonstrated all of these. When I had her extend and rotate her head to the right (Spurling's maneuver), that "shoulder blade" pain lit up like a Christmas tree. The problem wasn't her shoulder blade at all—it was her C5-6 segment sending false signals.
Why Understanding This Matters for Your Treatment
Here's why this distinction is so important: if you only treat the shoulder blade where you feel the pain, you're chasing symptoms, not solving the problem. It's like turning up your car radio to cover the sound of a grinding transmission—you haven't fixed anything.
Effective treatment requires addressing the cervical source:
1. Spinal Manipulation (Adjustments)
When we restore proper motion to restricted cervical segments, we reduce the aberrant signaling from irritated facet joints. A 2017 systematic review found that spinal manipulation provides significant pain relief for neck-related shoulder pain, likely by normalizing joint mechanoreceptor input and reducing nociceptive (pain) signaling.[6]
2. Trigger Point Therapy
Direct treatment of cervical muscle trigger points—using techniques like ischemic compression, dry needling, or instrument-assisted soft tissue mobilization—can deactivate the trigger point and eliminate the referred pain pattern.[7] In Sarah's case, three sessions of trigger point therapy to her levator scapulae dramatically reduced her interscapular symptoms.
3. Postural Correction and Ergonomics
Forward head posture (which worsens after MVAs due to protective muscle guarding) increases strain on cervical facets and perpetuates the pain cycle. We work on restoring neutral head position and proper ergonomics to reduce mechanical stress on sensitized tissues.
4. Neurodynamic Exercises
Gentle nerve gliding exercises help reduce neural sensitivity and restore normal nerve mechanics. These aren't about "unsticking" nerves—we're reducing the inflammatory environment around the nerve and improving its tolerance to movement.[8]
The Misdiagnosis Problem
This is where things get tricky for patients navigating the personal injury system. If your treating physician doesn't understand referred pain patterns, you might get diagnosed with:
- "Shoulder strain" (when it's actually cervical facet syndrome)
- "Rotator cuff tendinitis" (when it's actually C5-6 radiculopathy)
- "Muscle spasm" (when it's actually trigger point referral from cervical muscles)
These misdiagnoses lead to inappropriate treatment (you'll get shoulder therapy when you need cervical care) and can create problems with your personal injury claim. Insurance adjusters love to argue that shoulder blade pain isn't related to a neck injury when the mechanism doesn't make sense to them.
This is why accurate documentation matters. When we examine you, we're not just asking where it hurts—we're mapping the pain referral patterns, correlating them with specific cervical findings, and documenting the mechanism that explains why your shoulder blade hurts when the problem is in your neck.
The Science Behind the Sensation
For those who want to understand the neuroscience more deeply:
Convergence-Projection Theory
This is the leading explanation for referred pain. Visceral (organ) and somatic (musculoskeletal) afferent nerve fibers converge onto the same second-order neurons in the spinal cord. When your brain receives signals from these convergent neurons, it projects the sensation to the somatic (body surface) reference area because that's the most common source of pain your brain has experienced from that neural pathway.[9]
In practical terms: your brain has a lot of experience with shoulder blade muscle pain (you've slept wrong, carried heavy backpacks, etc.). It has less experience with C5-6 facet joint pain. So when those convergent signals arrive, your brain defaults to the familiar interpretation: "This must be shoulder blade pain."
Central Sensitization
In chronic cases, the spinal cord neurons themselves become hyperexcitable. This means they fire more easily and for longer durations in response to normally non-painful stimuli. You might develop a "pain memory" where your shoulder blade hurts even after the original cervical injury has healed, because the central nervous system has maintained the abnormal signaling pattern.[10]
This is one reason why early, appropriate treatment matters—we want to prevent this central sensitization from establishing itself.
What This Means for Your Recovery
If you're dealing with shoulder blade pain after a motor vehicle accident, here's what you should know:
1. Location Doesn't Always Equal Source
Just because your shoulder blade hurts doesn't mean that's where the problem is. A comprehensive examination should assess your entire cervical spine, not just poke around your scapula.
2. The Pattern Tells the Story
Pay attention to what makes your pain worse or better. If neck movements change your shoulder blade symptoms, that's a strong indicator of cervical origin.
3. Treatment Should Target the Source
If your provider is only treating your shoulder blade without addressing your neck, you're likely missing the primary driver of your symptoms.
4. Documentation is Critical
For personal injury cases, make sure your provider is documenting the referred pain pattern and explaining the connection to your cervical injury. This prevents insurance companies from arguing that your shoulder blade complaints are unrelated to your neck injury.
Sarah's Outcome
After eight weeks of treatment focused on her cervical spine—including specific adjustments to restore C5-6 motion, trigger point therapy to her levator scapulae, and postural correction exercises—Sarah's shoulder blade pain resolved completely. Her final exam showed restored cervical range of motion, no trigger point tenderness, and a negative Spurling's test.
"I can't believe the problem was in my neck the whole time," she said. "I kept trying to stretch my shoulder blade, and it did nothing. Once we started working on my neck, everything changed."
That's the power of understanding referred pain patterns. Treat the source, not just the symptom.
---
Key Takeaways
- Referred pain occurs when nerve signals from one area are interpreted by your brain as coming from another location
- Cervical facet joints, discs, and muscles commonly refer pain to the shoulder blade region
- Motor vehicle accidents create the perfect conditions for this referral pattern through facet irritation, muscle guarding, and nerve sensitization
- Effective treatment requires addressing the cervical source, not just the referred pain location
- Proper diagnosis and documentation of referred pain patterns is critical for personal injury claims
If you're experiencing shoulder blade pain after a car accident, especially if it changes with neck movements, you may be dealing with referred pain from your cervical spine. A thorough examination can identify the true source and guide appropriate treatment.
---
References
[1] Bogduk N. The anatomy and pathophysiology of neck pain. Phys Med Rehabil Clin N Am. 2011;22(3):367-382. https://pubmed.ncbi.nlm.nih.gov/21824583/
[2] Dwyer A, Aprill C, Bogduk N. Cervical zygapophyseal joint pain patterns. I: A study in normal volunteers. Spine. 1990;15(6):453-457. https://pubmed.ncbi.nlm.nih.gov/2402682/
[3] Panjabi MM, Cholewicki J, Nibu K, et al. Capsular ligament stretches during in vitro whiplash simulations. J Spinal Disord. 1998;11(3):227-232. https://pubmed.ncbi.nlm.nih.gov/9657546/
[4] Simons DG, Travell JG, Simons LS. Travell & Simons' Myofascial Pain and Dysfunction: The Trigger Point Manual. Vol 1. 2nd ed. Baltimore: Williams & Wilkins; 1999.
[5] Curatolo M, Bogduk N, Ivancic PC, et al. The role of tissue damage in whiplash-associated disorders: discussion paper 1. Spine. 2011;36(25 Suppl):S309-S315. https://pubmed.ncbi.nlm.nih.gov/22020605/
[6] Hidalgo B, Hall T, Bossert J, et al. The efficacy of manual therapy and exercise for treating non-specific neck pain: A systematic review. J Back Musculoskelet Rehabil. 2017;30(6):1149-1169. https://pubmed.ncbi.nlm.nih.gov/28826164/
[7] Fernández-de-Las-Peñas C, Alonso-Blanco C, Miangolarra JC. Myofascial trigger points in subjects presenting with mechanical neck pain: a blinded, controlled study. Man Ther. 2007;12(1):29-33. https://pubmed.ncbi.nlm.nih.gov/16777467/
[8] Nee RJ, Butler D. Management of peripheral neuropathic pain: Integrating neurobiology, neurodynamics, and clinical evidence. Phys Ther Sport. 2006;7(1):36-49.
[9] Arendt-Nielsen L, Svensson P. Referred muscle pain: basic and clinical findings. Clin J Pain. 2001;17(1):11-19. https://pubmed.ncbi.nlm.nih.gov/11289084/
[10] Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2-S15. https://pubmed.ncbi.nlm.nih.gov/20961685/
---
Dr. Ryan Todd Lloyd is a Qualified Medical Examiner and chiropractor specializing in personal injury cases in Petaluma, California. His practice focuses on evidence-based treatment of motor vehicle accident injuries, with particular expertise in complex pain patterns and their biomechanical origins.
